
eMedicine emerg/31 | ICD-10 I24.9 MeSH D054058 | |
 | ||
Patient UK Acute coronary syndrome | ||
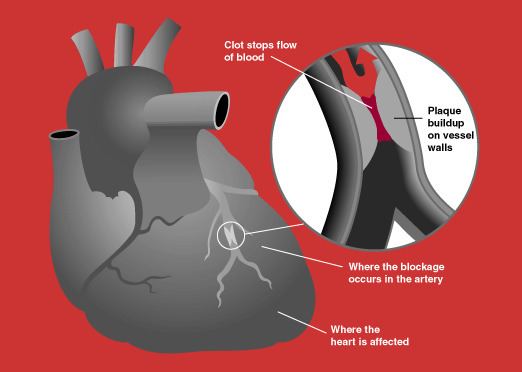
Acute coronary syndrome (ACS) is a syndrome (set of signs and symptoms) due to decreased blood flow in the coronary arteries such that part of the heart muscle is unable to function properly or dies. The most common symptom is chest pain, often radiating to the left arm or angle of the jaw, pressure-like in character, and associated with nausea and sweating. Acute coronary syndrome is usually caused by one of three problems: ST elevation myocardial infarction (STEMI, 30%), non ST elevation myocardial infarction (NSTEMI, 25%), or unstable angina (38%).
Contents
- Signs and symptoms
- Electrocardiogram
- Imaging and blood tests
- Prediction scores
- Prevention
- Treatment
- STEMI
- NSTEMI and NSTE ACS
- TIMI score
- Biomarkers for diagnosis
- Biomarkers for risk determination
- Day of admission
- References
These types are named according to the appearance of the electrocardiogram (ECG/EKG) as non-ST segment elevation myocardial infarction and ST segment elevation myocardial infarction. There can be some variation as to which forms of myocardial infarction (MI) are classified under acute coronary syndrome.
ACS should be distinguished from stable angina, which develops during exertion and resolves at rest. In contrast with stable angina, unstable angina occurs suddenly, often at rest or with minimal exertion, or at lesser degrees of exertion than the individual's previous angina ("crescendo angina"). New onset angina is also considered unstable angina, since it suggests a new problem in a coronary artery.
Though ACS is usually associated with coronary thrombosis, it can also be associated with cocaine use. Cardiac chest pain can also be precipitated by anemia, bradycardias (excessively slow heart rate) or tachycardias (excessively fast heart rate).
Signs and symptoms
The cardinal symptom of decreased blood flow to the heart is chest pain, experienced as tightness around the chest and radiating to the left arm and the left angle of the jaw. This may be associated with diaphoresis (sweating), nausea and vomiting, as well as shortness of breath. In many cases, the sensation is "atypical", with pain experienced in different ways or even being completely absent (which is more likely in female patients and those with diabetes). Some may report palpitations, anxiety or a sense of impending doom (angor animi) and a feeling of being acutely ill.
The description of the chest discomfort as a pressure has little utility in aiding a diagnosis as it is not specific for ACS.
Electrocardiogram
In the setting of acute chest pain, the electrocardiogram is the investigation that most reliably distinguishes between various causes. The ECG should be done as early as practicable, including in the ambulance if possible. If this indicates acute heart damage (elevation in the ST segment, new left bundle branch block), treatment for a heart attack in the form of angioplasty or thrombolysis is indicated immediately (see below). In the absence of such changes, it is not possible to immediately distinguish between unstable angina and NSTEMI.
Imaging and blood tests
As it is only one of the many potential causes of chest pain, the patient usually has a number of tests in the emergency department, such as a chest X-ray, blood tests (including myocardial markers such as troponin I or T, and H-FABP and/or a D-dimer if a pulmonary embolism is suspected), and telemetry (monitoring of the heart rhythm).
Prediction scores
The ACI-TIPI score can be used to aid diagnosis; using seven variables from the admission record, this score predicts crudely which patients are likely to have myocardial ischemia. For example, according to a randomized controlled trial, males having chest pain with normal or non diagnostic ECG are at higher risk for having acute coronary syndrome than women. In this study, the sensitivity was 65.2% and specificity was 44%. This particular study had an 8.4% prevalence of acute coronary syndrome, which means the positive predictive value of being a male with chest pain and having coronary syndrome is 9.6% and negative predictive value is 93.2% ( click here to adjust these results for patients at higher or lower risk of acute coronary syndrome).
In a second cohort study, exercise electrocardiography was similarly found to be a poor predictor of acute coronary syndrome at follow-up. Of the patients who had a coronary event at 6 years of follow up, 47% had a negative ECG at the start of the study. With an average follow up of 2.21 years the receiver operating characteristic curves gave resting ECG a score of 0.72 and exercise ECG a score of 0.74.
There are not only prediction scores for diagnosis of ACS, but also prognosis. Most notably, the GRACE ACS Risk and Mortality score helps diagnose, and based upon that score predicts mortality rate of a given patient. It takes into account both clinical (blood pressure, heart rate, EKG findings) and medical history in its scoring system.
Prevention
Acute coronary syndrome often reflects a degree of damage to the coronaries by atherosclerosis. Primary prevention of atherosclerosis is controlling the risk factors: healthy eating, exercise, treatment for hypertension and diabetes, avoiding smoking and controlling cholesterol levels; in patients with significant risk factors, aspirin has been shown to reduce the risk of cardiovascular events. Secondary prevention is discussed in myocardial infarction.
After a ban on smoking in all enclosed public places was introduced in Scotland in March 2006, there was a 17% reduction in hospital admissions for acute coronary syndrome. 67% of the decrease occurred in non-smokers.
Treatment
People with presumed ACS are typically treated with aspirin, clopidogrel or ticagrelor, nitroglycerin, and if the chest discomfort persists morphine. Other analgesics such as nitrous oxide are of unknown benefit. Angiography is recommended in those who have either new ST elevation or a new left bundle branch block on their ECG. Unless the person has low oxygen levels additional oxygen does not appear to be useful.
STEMI
If the ECG confirms changes suggestive of myocardial infarction (ST elevations in specific leads, a new left bundle branch block or a true posterior MI pattern), thrombolytics may be administered or primary coronary angioplasty may be performed. In the former, medication is injected that stimulates fibrinolysis, destroying blood clots obstructing the coronary arteries. In the latter, a flexible catheter is passed via the femoral or radial arteries and advanced to the heart to identify blockages in the coronaries. When occlusions are found, they can be intervened upon mechanically with angioplasty and usually stent deployment if a lesion, termed the culprit lesion, is thought to be causing myocardial damage. Data suggest that rapid triage, transfer and treatment is essential. The time frame for door-to-needle thrombolytic administration according to American College of Cardiology (ACC) guidelines should be within 30 minutes, whereas the door-to-balloon Percutaneous Coronary Intervention (PCI) time should be less than 90 minutes. It was found that thrombolysis is more likely to be delivered within the established ACC guidelines among patients with STEMI as compared to PCI according to a case control study.
NSTEMI and NSTE-ACS
If the ECG does not show typical changes, the term "non-ST segment elevation ACS" is applied. The patient may still have suffered a "non-ST elevation MI" (NSTEMI). The accepted management of unstable angina and acute coronary syndrome is therefore empirical treatment with aspirin, a second platelet inhibitor such as clopidogrel, prasugrel or ticagrelor, and heparin (usually a low-molecular weight heparin such as enoxaparin), with intravenous glyceryl trinitrate and opioids if the pain persists.
A blood test is generally performed for cardiac troponins twelve hours after onset of the pain. If this is positive, coronary angiography is typically performed on an urgent basis, as this is highly predictive of a heart attack in the near-future. If the troponin is negative, a treadmill exercise test or a thallium scintigram may be requested.
If there is no evidence of ST segment elevation on the electrocardiogram, delaying urgent angioplasty until the next morning is not inferior to doing so immediately. Using statins in the first 14 days after ACS reduces the risk of further ACS.
In a cohort study comparing NSTEMI and STEMI, patients with NSTEMI had statistically similar mortality at one year after PCI as compared to patients with STEMI (3.4% vs 4.4%). However, NSTEMI had significantly more "major cardiac events" (death, myocardial infarction, disabling stroke, or requiring revascularization) at one year (24.0% vs 16.6%).
Cocaine associated ACS should be managed in a manner similar to other patients with acute coronary syndrome except beta blockers should not be used and benzodiazepines should be administered early.
TIMI score
The TIMI risk score can identify high risk patients and has been independently validated.
Biomarkers for diagnosis
The aim of diagnostic markers is to identify patients with ACS even when there is no evidence of heart muscle damage.
Biomarkers for risk determination
The aim of prognostic markers is to reflect different components of pathophysiology of ACS. For example:
Day of admission
Studies have shown that for ACS patients, weekend admission is associated with higher mortality and lower utilization of invasive cardiac procedures, and those who did undergo these interventions had higher rates of mortality and complications than their weekday counterparts. This data leads to the possible conclusion that access to diagnostic/interventional procedures may be contingent upon the day of admission, which may impact mortality. This phenomenon is described as weekend effect.