
 | ||
Thyroplasty is a phonosurgical technique designed to improve the voice by altering the thyroid cartilage of the larynx (the voice box), which houses the vocal cords in order to change the position or the length of the vocal cords.
Contents
Types
There are four different types of thyroplasty procedures described by Isshiki:
Type 1 thyroplasty (medialization thyroplasty)
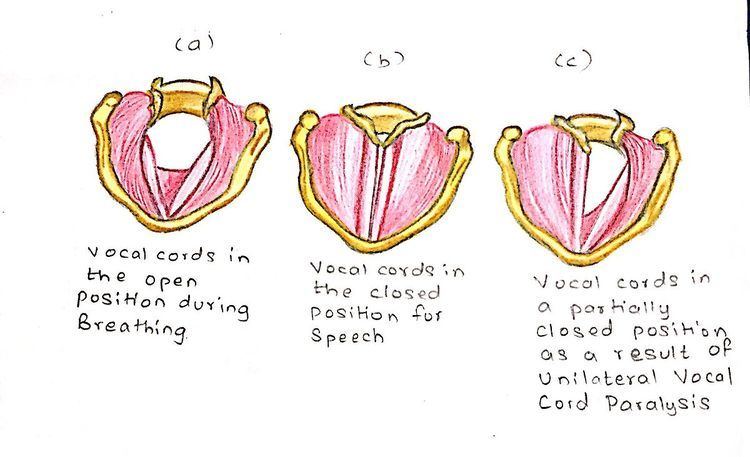
It is the most commonly used surgical procedure to correct unilateral vocal cord paralysis (a condition where the vocal cord of one side is paralysed).
Procedure
In this type of thyroplasty, a rectangular portion of the thyroid cartilage is mobilized and pushed towards the medial side using a piece of silastic block of proper shape under local anesthesia.
Earlier, the piece of the thyroid cartilage was kept along with implant and the stitches were taken, but nowadays, the piece of the thyroid cartilage is cut and removed to avoid complications.
Types of procedures
Currently, there are four types of implant procedures which are used to perform type 1 thyroplasty.
This system was discovered after years of research and the main advantage of this implant system is that it eliminates the process of customizing the implant at the time of surgery.This system consists of different sizes and shapes of shims made of silastic. It has the most proven success rate and the duration of the procedure is slow in comparison to other implant system.The other advantage is that it does not require suturing. It has reduced incidence of trauma.
This system consists of different sizes and shapes of implants made from hydroxyapatite (a naturally occurring mineral form of calcium apatite). It helps in achieving accurate vocal fold medialization. This procedure is technically reversible. But it should be used in candidates of permanent implantation due to its biocompatible clinical use lasting for nearly a decade.
This system generally consists of two sizes of implants made out of pure titanium. It has a lot of advantages and the main one is that it reduces the operative time. Titanium is more safe than other implants. It has great biocompatibility. The implants are available in only two variants and they are designed in such a way that they ensure optimal fixation. The implant can be easily made as the titanium sheet is easy to shape. The technique is relatively simple and does not require expensive instruments.
In this type of implant system, the implant is made of homopolymer of polytetrafluoroethylene in form of minute beads arranged in a fine fiber mesh. It is malleable and can be inserted through a small window.
Indications
Contraindications
Complications
Advantages
Disadvantages
Limitations
Type 2 thyroplasty (lateralization thyroplasty)
It is a surgical procedure used in conditions like adductor spasmodic dysphonia (a condition in which there is distortion of the voice due to excessively tight closure of the glottis on phonation). Generally, lateralization thyroplasty is intended to prevent this tight closure of the glottis at the terminal stage of phonation by lateralizing the position of the vocal cord. This is a completely mechanical process.
Procedure
An incision is made at midline of the thyroid cartilage. A silicon wedge is used to fix the incised thyroid cartilage in the newly abducted position.
Modified technique
A specially deviced titanium bridge is used instead of silicon wedge. Nowadays, instead of one titanium bridge, two titanium bridges are used for permanent fixation of the thyroid cartilage.
Indications
Contraindications
Type 3 thyroplasty (relaxation thyroplasty)
This procedure is generally done to lower the vocal pitch by shortening the thyroid ala.
Procedure
In this thyroplasty, the relaxation of the vocal cords is done by antero-posterior shortening of the thyroid ala.
Indications
Procedure
This procedure is done to elevate the vocal pitch. This procedure consists of lengthening of the thyroid cartilage. It includes cricothyroid approximation.
Indications
Combination
In some specific conditions, different types of thyroplasties are combined for the desired results.
Purpose
The main purpose of this combination is the medialization of the entire vocal cord (anterior and posterior).