
 | ||
In psychology, the theory of planned behavior (abbreviated TPB) is a theory that links beliefs and behavior. The concept was proposed by Icek Ajzen to improve on the predictive power of the theory of reasoned action by including perceived behavioural control. It is a theory explaining human behaviour. It has been applied to studies of the relations among beliefs, attitudes, behavioral intentions and behaviors in various fields such as advertising, public relations, advertising campaigns and healthcare.
Contents
- Extension from the theory of reasoned action
- Extension of self efficacy
- Normative beliefs and subjective norms
- Control beliefs and perceived behavioral control
- Behavioral intention and behavior
- Perceived behavioral control vs self efficacy
- Attitude toward behavior vs outcome expectancy
- Social influence
- Model
- Formula
- Strengths
- Limitations
- Applications of the theory
- References
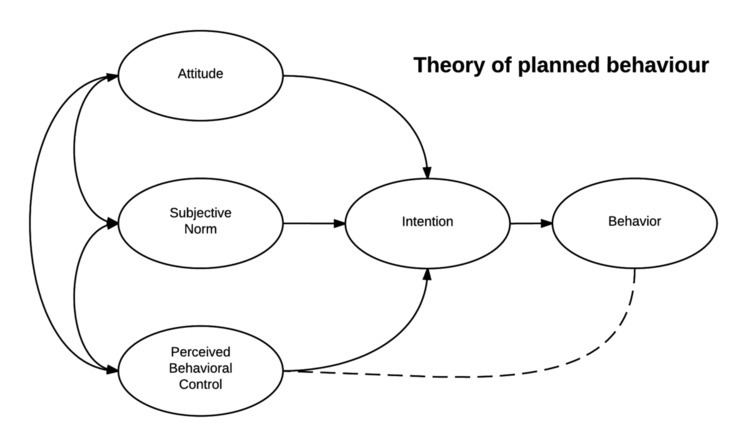
The theory states that attitude toward behavior, subjective norms, and perceived behavioral control, together shape an individual's behavioral intentions and behaviors.
Extension from the theory of reasoned action
The theory of planned behavior was proposed by Icek Ajzen in 1985 through his article "From intentions to actions: A theory of planned behavior." The theory was developed from the theory of reasoned action, which was proposed by Martin Fishbein together with Icek Ajzen in 1980. The theory of reasoned action was in turn grounded in various theories of attitude such as learning theories, expectancy-value theories, consistency theories (such as Heider's balance theory, Osgood and Tannenbaum's congruity theory, and Festinger's dissonance theory) and attribution theory. According to the theory of reasoned action, if people evaluate the suggested behavior as positive (attitude), and if they think their significant others want them to perform the behavior (subjective norm), this results in a higher intention (motivations) and they are more likely to do so. A high correlation of attitudes and subjective norms to behavioral intention, and subsequently to behavior, has been confirmed in many studies.
A counter-argument against the high relationship between behavioral intention and actual behavior has also been proposed, as the results of some studies show that, because of circumstantial limitations, behavioral intention does not always lead to actual behavior. Namely, since behavioral intention cannot be the exclusive determinant of behavior where an individual's control over the behavior is incomplete, Ajzen introduced the theory of planned behavior by adding a new component, "perceived behavioral control". By this, he extended the theory of reasoned action to cover non-volitional behaviors for predicting behavioral intention and actual behavior.
The most recent addition of a third factor, perceived behavioral control, refers to the degree to which a person believes that they control any given behavior (class notes). The theory of planned behavior suggests that people are much more likely to intend to enact certain behaviors when they feel that they can enact them successfully. Increased perceived behavioral control is a mix of two dimensions: self-efficacy and controllability (170). Self-efficacy refers to the level of difficulty that is required to perform the behavior, or one's belief in their own ability to succeed in performing the behavior. Controllability refers to the outside factors, and one's belief that they personally have control over the performance of the behavior, or if it is controlled by externally, uncontrollable factors. If a person has high perceived behavioral control, then they have an increased confidence that they are capable of performing the specific behavior successfully.
The theory has since been improved and renamed the reasoned action approach by Azjen and his colleague Martin Fishbein.
Extension of self-efficacy
In addition to attitudes and subjective norms (which make the theory of reasoned action), the theory of planned behavior adds the concept of perceived behavioral control, which originates from self-efficacy theory (SET). Self-efficacy was proposed by Bandura in 1977, which came from social cognitive theory. According to Bandura, expectations such as motivation, performance, and feelings of frustration associated with repeated failures determine effect and behavioral reactions. Bandura separated expectations into two distinct types: self-efficacy and outcome expectancy. He defined self-efficacy as the conviction that one can successfully execute the behavior required to produce the outcomes. The outcome expectancy refers to a person's estimation that a given behavior will lead to certain outcomes. He states that self-efficacy is the most important precondition for behavioral change, since it determines the initiation of coping behavior. Previous investigations have shown that peoples' behavior is strongly influenced by their confidence in their ability to perform that behavior. As the self-efficacy theory contributes to explaining various relationships between beliefs, attitudes, intentions, and behavior, the SET has been widely applied to health-related fields such as physical activity and mental health in preadolescents, and exercise.
Normative beliefs and subjective norms
Control beliefs and perceived behavioral control
Behavioral intention and behavior
Perceived behavioral control vs. self-efficacy
As Ajzen (1991) stated in the theory of planned behavior, knowledge of the role of perceived behavioral control came from Bandura's concept of self-efficacy. More recently, Fishbein and Cappella stated that self-efficacy is the same as perceived behavioral control in his integrative model, which is also measured by items of self-efficacy in a previous study.
In previous studies, the construction and the number of item inventory of perceived behavioral control have depended on each particular health topic. For example, for smoking topics, it is usually measured by items such as "I don't think I am addicted because I can really just not smoke and not crave for it," and "It would be really easy for me to quit."
The concept of self-efficacy is rooted in Bandura's social cognitive theory. It refers to the conviction that one can successfully execute the behavior required to produce the outcome. The concept of self-efficacy is used as perceived behavioral control, which means the perception of the ease or difficulty of the particular behavior. It is linked to control beliefs, which refers to beliefs about the presence of factors that may facilitate or impede performance of the behavior.
It is usually measured with items which begins with the stem, "I am sure I can ... (e.g., exercise, quit smoking, etc.)" through a self-report instrument in their questionnaires. Namely, it tries to measure the confidence toward the probability, feasibility, or likelihood of executing given behavior.
Attitude toward behavior vs. outcome expectancy
The theory of planned behavior specifies the nature of relationships between beliefs and attitudes. According to these models, people's evaluations of, or attitudes toward behavior are determined by their accessible beliefs about the behavior, where a belief is defined as the subjective probability that the behavior will produce a certain outcome. Specifically, the evaluation of each outcome contributes to the attitude in direct proportion to the person's subjective possibility that the behavior produces the outcome in question.
Outcome expectancy was originated from the expectancy-value model. It is a variable-linking belief, attitude, opinion and expectation. The theory of planned behavior's positive evaluation of self-performance of the particular behavior is similar to the concept to perceived benefits, which refers to beliefs regarding the effectiveness of the proposed preventive behavior in reducing the vulnerability to the negative outcomes, whereas their negative evaluation of self-performance is similar to perceived barriers, which refers to evaluation of potential negative consequences that might result from the enactment of the espoused health behavior.
Social influence
The concept of social influence has been assessed by social norm and normative belief in both the theory of reasoned action and theory of planned behavior. Individuals' elaborative thoughts on subjective norms are perceptions on whether they are expected by their friends, family and the society to perform the recommended behavior. Social influence is measured by evaluation of various social groups. For example, in the case of smoking:
- Subjective norms from the peer group include thoughts such as, "Most of my friends smoke," or "I feel ashamed of smoking in front of a group of friends who don't smoke";
- Subjective norms from the family include thoughts such as, "All of my family smokes, and it seems natural to start smoking," or "My parents were really mad at me when I started smoking"; and
- Subjective norms from society or culture include thoughts such as, "Everyone is against smoking," and "We just assume everyone is a nonsmoker."
While most models are conceptualized within individual cognitive space, the theory of planned behavior considers social influence such as social norm and normative belief, based on collectivistic culture-related variables. Given that an individual's behavior (e.g., health-related decision-making such as diet, condom use, quitting smoking and drinking, etc.) might very well be located in and dependent on the social networks and organization (e.g., peer group, family, school and workplace), social influence has been a welcomed addition.
Model
Human behavior is guided by three kinds of consideration, "behavioral beliefs," "normative beliefs," and "control beliefs." In their respective aggregates, "behavioral beliefs" produce a favorable or unfavorable "attitude toward the behavior"; "normative beliefs" result in "subjective norm"; and "control beliefs" gives rise to "perceived behavioral control."
In combination, "attitude toward the behavior," "subjective norm," and "perceived behavioral control" lead to the formation of a "behavioral intention". In particular, "perceived behavioral control" is presumed to not only affect actual behavior directly, but also affect it indirectly through behavioral intention.
As a general rule, the more favorable the attitude toward behavior and subjective norm, and the greater the perceived behavioral control, the stronger the person's intention to perform the behavior in question should be. Finally, given a sufficient degree of actual control over the behavior, people are expected to carry out their intentions when the opportunity arises.
Formula
In its simplest form, the theory of planned behavior can be expressed as the following mathematical function:
BI = (W_1)AB[=Σ(b)(e)] + (W_2)SN[=Σ(n)(m)] + (W_3)PBC[=Σ(c)(p)]To the extent that it is an accurate reflection of actual behavioral control, perceived behavioral control can, together with intention, be used to predict behavior.
Strengths
The theory of planned behavior can cover people's non-volitional behavior which cannot be explained by the theory of reasoned action.
An individual's behavioral intention cannot be the exclusive determinant of behavior where an individual's control over the behavior is incomplete. By adding "perceived behavioral control," the theory of planned behavior can explain the relationship between behavioral intention and actual behavior.
Several studies found that the TPB would help better predict health-related behavioral intention than the theory of reasoned action. The TPB has improved the predictability of intention in various health-related fields such as condom use, leisure, exercise, diet, etc.
In addition, the theory of planned behavior as well as the theory of reasoned action can explain the individual's social behavior by considering "social norm" as an important variable.
Limitations
Some scholars claim that the theory of planned behavior is based on cognitive processing and have criticised the theory on those grounds. However, there is nothing in the theory that states that attitudes are formed consciously or that evaluation of beliefs, for example is not influenced by emotion. The theory says nothing about where beliefs and their evaluations come from, hence claims that it excludes emotion are without foundation in fact. Nevertheless, critics continue to make these unfounded complaints.
Clearly, many behaviors may be largely influenced by emotion. However, this is not necessarily a drawback for predicting these behaviors, contrary to some complaints. Strong emotions are relevant to this model because they can influence beliefs and other constructs in this model. Poor predictability for health-related behavior in previous health research may be attributed to poor application of the model, associated methods and measures. Most of the research is correlational, and more evidence based on experimental studies is welcome although experiments, by nature, lack external validity because they prioritize internal validity.
Applications of the theory
So far, the theory of planned behavior has more than 1200 research bibliographies in academic databases such as Communication & Mass Media Complete, Academic Search Premier, PsycARTICLES, Business Source Premier, PsycINFO, and PsycCRITIQUES.
In particular, recently, several studies found that the TPB would better help to predict health-related behavioral intention than the theory of reasoned action (TRA) given that the TPB has improved the predictability of intention in various health-related fields such as condom use, leisure, exercise, and diet.
The Theory of Planned Behavior has been applied to study a range of pro-social behaviors, such as charitable giving. In one study, the TPB explained nearly 70% of the variance in intentions to donate to charity. However, the TPB also shows good applicability in regards to antisocial behaviours, such as using deception in the online environment.
Another application of the theory of planned behavior is in the field of environmental psychology. Generally speaking, actions that are environmentally friendly carry a positive normative belief. That is to say, sustainable behaviors are widely promoted as positive behaviors. However, although there may be a behavioral intention to practice such behaviors, perceived behavioral control can be hindered by constraints such as a belief that one's behavior will not have any impact. For example, if one intends to behave in an environmentally responsible way but there is a lack of accessible recycling infrastructure, perceived behavioral control is low, and constraints are high, so the behavior may not occur. Applying the theory of planned behavior in these situations helps explain contradictions between sustainable attitudes and unsustainable behavior.
The theory of planned behavior model is thus a very powerful and predictive model for explaining human behavior. That is why the health and nutrition fields have been using this model often in their research studies. In one study, utilizing the theory of planned behavior, the researchers determine obesity factors in overweight Chinese Americans. Intention to prevent becoming overweight was the key construct in the research process. It is important that nutrition educators provide the proper public policies in order to provide good tasting, low-cost, healthful food.
The Theory of Planned Behavior can also be applied in area of applied nutrition intervention. In a recent study by Sweitzer, TPB (in conjunction with SCT) was utilized to encourage parents to pack more fruits, vegetables and whole grains (FVWG) in sack lunches of preschool children. Behavioral constructs of TPD were used to develop intervention strategies. Knowledge/behavioral control, Self-efficacy/perceived behavioral control, subjective norms and intentions were measured to see effects on behavior. The results found a significant increase in vegetables and whole grains packed in lunches when interventions were planned using the TPB constructs. Psychosocial variables were useful predictors of lunch packing behaviors of parents and this study provided a divergent application of model-exploration of an area of parental behavior as a role in the development of young children’s dietary behaviors. In a study by McConnon, the application of the TPB was used to prevent weight regain in an overweight cohort who recently experienced a significant weight loss. Using the constructs of TPB, it was found that perceived need to control weight is the most positive predictor of behavior for weight maintenance. The TPB model can be used to predict weight gain prevention expectation in an overweight cohort. The TPB can also be utilized to measure behavioral intention of practitioners in promoting specific health behaviors. In this study by Chase, dietitians’ intentions to promote whole grain foods was studied. It was found that the strongest indicator of intention of dietitians to promote whole grain foods was the construct of normative beliefs with 97% of dietitians indicating that health professionals should promote whole grains and 89% wanted to comply with this belief. However, knowledge and self-efficacy of instituting this belief was faulted with only 60% of dietitians being able to correctly identify a whole grain product from a food label, 21% correctly identifying current recommendations and 42% of dietitians did not know there was a recommendation for whole grain consumption. Although the response rate to complete mailed surveys for this study was low (39%), the results provided preliminary data on the strong effect of normative beliefs on dietitian intentions to promote whole grain and the need for nutrition need for additional education for practicing dietitians focusing on increase knowledge and self-efficacy for promoting whole grains.
Important Steps in Application of the Theory
When applying the TPB as a theoretical framework, certain steps should be followed to promote increased validity of results. First, target behavior should be specified in terms of action, target, context, and time. For example, the goal might be to “consume at least one serving of whole grains during breakfast each day in the forthcoming month”. In this statement, “consuming” is the action, “one serving of whole grains” is the target, “during breakfast each day” is the context, and “in the forthcoming month” is the time. Once a goal is specified, an elicitation phase can be used to identify salient issues. The pertinent and central beliefs for a certain behavior may be very different for different populations. Therefore, conducting open-ended elicitation interviews is one of the most crucial steps in applying the TPB. Elicitation interviews help to identify relevant behavioral outcomes, referents, cultural factors, facilitators, and barriers for each particular behavior and target population under investigation. The following are sample questions that may be used during an elicitation interview:
What do you like/ dislike about behavior X? What are some disadvantages of doing behavior X? Who would be against your doing behavior X? Who can you think of that would do behavior X? What things make it hard for you to do behavior X? If you want to do behavior X, how certain are you that you can?
A questionnaire can then be designed, based on results from the elicitation interview, to measure model constructs with attention to cultural issues. After implementation of the questionnaire, thorough analyses should be conducted to assess whether the intervention influenced model constructs associated with intention and behavior. Results and findings from the analysis can be used to develop effective interventions for eliciting behavioral change, especially within nutrition and health.