
Group Group VI (ssRNA-RT) | Family Retroviridae | |
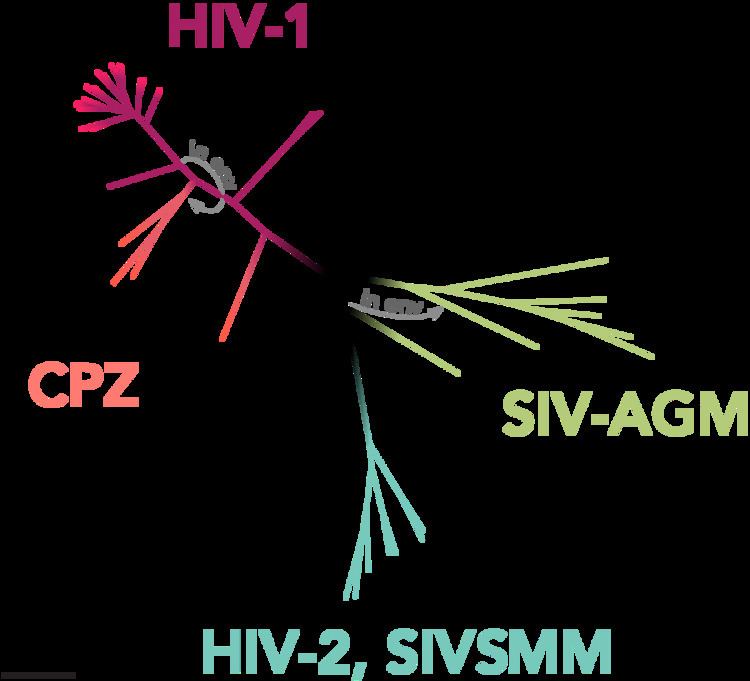 | ||
One of the obstacles to treatment of the human immunodeficiency virus is its high genetic variability. HIV can be divided into two major types, HIV type 1 (HIV-1) and HIV type 2 (HIV-2). HIV-1 is related to viruses found in chimpanzees and gorillas living in western Africa, while HIV-2 viruses are related to viruses found in the endangered west African primate sooty mangabey. HIV-1 viruses may be further divided into groups. The HIV-1 group M viruses predominate and are responsible for the AIDS pandemic. Group M can be further subdivided into subtypes based on genetic sequence data. Some of the subtypes are known to be more virulent or are resistant to different medications. Likewise, HIV-2 viruses are thought to be less virulent and transmissible than HIV-1 M group viruses, although HIV-2 is known to cause AIDS.
Contents
HIV-1
HIV-1 is the most common and pathogenic strain of the virus. Scientists divide HIV-1 into a major group (Group M) and two or more minor groups, namely Group N, O and possibly a group P. Each group is believed to represent an independent transmission of SIV into humans (but subtypes within a group are not). A total of 39 ORFs are found in all six possible reading frames (RFs) of HIV-1 complete genome sequence, but only a few of them are functional.
Group M
With 'M' for "major", this is by far the most common type of HIV, with more than 90% of HIV/AIDS cases deriving from infection with HIV-1 group M. The M group is subdivided further into clades, called subtypes, that are also given a letter. There are also "circulating recombinant forms" or CRFs derived from recombination between viruses of different subtypes which are each given a number. CRF12_BF, for example, is a recombination between subtypes B and F.
These subtypes are sometimes further split into sub-subtypes such as A1 and A2 or F1 and F2. In 2015, the strain CRF19, a recombinant of subtype A, subtype D and subtype G, with a subtype D protease, was found to be strongly associated with rapid progression to AIDS in Cuba. This is not thought to be a complete or final list, and further types are likely to be found.
Group N
The 'N' stands for "non-M, non-O". This group was discovered by a Franco-Cameroonia team in 1998, when they identified and isolated the HIV-1 variant strain, YBF380, from a Cameroonian woman who died of AIDS in 1995. When tested, the YBF380 variant reacted with an envelope antigen from SIVcpz rather than with those of Group M or Group O, indicating it was indeed a novel strain of HIV-1. As of 2015, less than 20 Group N infections have been recorded.
Group O
The O ("Outlier") group is not usually seen outside of West-central Africa. It is reportedly most common in Cameroon, where a 1997 survey found that about 2% of HIV-positive samples were from Group O. The group caused some concern because it could not be detected by early versions of the HIV-1 test kits. More advanced HIV tests have now been developed to detect both Group O and Group N.
Group P
In 2009, a newly analyzed HIV sequence was reported to have greater similarity to a simian immunodeficiency virus recently discovered in wild gorillas (SIVgor) than to SIVs from chimpanzees (SIVcpz). The virus had been isolated from a Cameroonian woman residing in France who was diagnosed with HIV-1 infection in 2004. The scientists reporting this sequence placed it in a proposed Group P "pending the identification of further human cases".
HIV-2 has not been widely recognized outside of Africa. The first case in the United States was in 1987. Many test kits for HIV-1 will also detect HIV-2.
As of 2010, there are 8 known HIV-2 groups (A to H). Of these, only groups A and B are pandemic. Group A is found mainly in West Africa, but has also spread globally to Angola, Mozambique, Brazil, India, Europe and the US. Despite the presence of HIV-2 globally, Group B is mainly confined to West Africa. Despite its relative confinement, HIV-2 should be considered in all patients exhibiting symptoms of HIV that not only come from West Africa, but also anyone who has had any body fluid transfer with a person from West Africa (i.e. needle sharing, sexual contact, etc.).
HIV-2 is closely related to simian immunodeficiency virus endemic in sooty mangabeys (Cercocebus atys atys) (SIVsmm), a monkey species inhabiting the forests of Littoral West Africa. Phylogenetic analyses show that the virus most closely related to the two strains of HIV-2 which spread considerably in humans (HIV-2 groups A and B) is the SIVsmm found in the sooty mangabeys of the Tai forest, in western Ivory Coast.
There are six additional known HIV-2 groups, each having been found in just one person. They all seem to derive from independent transmissions from sooty mangabeys to humans. Groups C and D have been found in two people from Liberia, groups E and F have been discovered in two people from Sierra Leone, and groups G and H have been detected in two people from the Ivory Coast. Each of these HIV-2 strains, for which humans are probably dead-end hosts, is most closely related to SIVsmm strains from sooty mangabeys living in the same country where the human infection was found.
Diagnosis
HIV-2 diagnosis can be made when a patient has no symptoms but positive blood work indicating the individual has HIV. The Multispot HIV-1/HIV-2 Rapid Test is currently the only FDA approved method for such differentiation between the two viruses. Recommendations for the screening and diagnosis of HIV has always been to use enzyme immunoassays that detect HIV-1, HIV-1 group O, and HIV-2. When screening the combination, if the test is positive followed by an indeterminate HIV-1 western blot, a follow up test, such as amino acid testing, must be performed to distinguish which infection is present. According to the NIH, a differential diagnosis of HIV-2 should be considered when a person is of West African descent or has had sexual contact or shared needles with such a person. West Africa is at the highest risk as it is the origin of the virus.
Treatments
HIV-2 has been found to be less pathogenic than HIV-1. The mechanism of HIV-2 is not clearly defined, nor the difference from HIV-1, however the transmission rate is much lower in HIV-2 than HIV-1. Both infections can lead to AIDS in affected individuals and both can mutate to develop drug resistance. Disease Monitoring in patients with HIV-2 includes clinical evaluation and CD4 cell counts, while treatment includes Anti-Retroviral Therapy (ART), Nucleoside Reverse Transcriptase Inhibitors (NRTIs), Protease Inhibitors (PI), and Non-Nucleoside Reverse Transcriptase Inhibitors (NNRTIs) with the addition of CCR5 co-receptor antagonists and fusion inhibitors.
Choice of initial and/or second-line therapy for HIV-2 has not yet been defined. HIV-2 appears to be resistant to NNRTIs intrinsically, but may be sensitive to NRTIs, though the mechanism is poorly understood. Protease inhibitors have shown variable effect, while integrase inhibitors are also being evaluated. Combination regimens of the above listed therapies are being looked into as well, also showing variable effect depending on the types of therapies combined. While the mechanisms are not clearly understood for HIV-1 and HIV-2, it is known that they use different pathways and patterns, making the algorithms used to evaluate HIV-1 resistance-associated mutations irrelevant to HIV-2.
Each virus can be contracted individually, or they can be contracted together in what is referred to as co-infection. HIV-2 seems to have lower mortality rates, less severe symptoms and slower progression to AIDS than HIV-1 alone or the co-infection. In co-infection, however, this is largely dependent on which virus was contracted first. HIV-1 tends to out compete HIV-2 for disease progression. Co-infection seems to be a growing problem globally as time progresses, with most cases being identified in West African countries, as well as some cases in the US.
Pregnancy
If a pregnant mother is exposed, screening is performed as normal. If HIV-2 is present, a number of perinatal ART drugs may be given as a prophylactic to lower the risk of mother-to-child transmission. After the child is born, a standard 6-week regimen of these prophylactics should be initiated. Breast milk may also contain particles of HIV-2; therefore, breastfeeding is strictly advised against.
Evolution
HIV is evolving to a milder form but is "an awfully long way" from no longer being deadly.
Drug resistance mutations
Isolates of HIV-1 and HIV-2 with resistance to antiretroviral drugs arise through natural selection and genetic mutations, which have been tracked and analyzed. The Stanford HIV Drug Resistance Database and the International AIDS Society publish lists of the most important of these; first year listing 80 common mutations, and the latest year 93 common mutations, and made available through the Stanford HIV RT and Protease Sequence Database.