
Specialty neurology ICD-9-CM 335.1 DiseasesDB 7144 | ICD-10 G12.1 OMIM 313200 eMedicine article/1172604 | |
 | ||
Spinal and bulbar muscular atrophy (SBMA), also known as spinobulbar muscular atrophy, bulbo-spinal atrophy, X-linked bulbospinal neuropathy (XBSN), X-linked spinal muscular atrophy type 1 (SMAX1), Kennedy's disease (KD), and many other names, is a debilitating neurodegenerative disorder resulting in muscle cramps and progressive weakness due to degeneration of motor neurons in the brain stem and spinal cord.
Contents
- Signs and symptoms
- Neuromuscular
- Homozygous females
- Genetics
- Pathophysiology
- Diagnosis
- Management
- Prognosis
- History
- References
The condition is associated with mutation of the androgen receptor (AR) gene and is inherited in an X-linked recessive manner. As with many genetic disorders, no cure is known, although research continues. Because of its endocrine manifestations related to the impairment of the AR gene, SBMA can be viewed as a variation of the disorders of the androgen insensitivity syndrome (AIS). It is also related to other neurodegenerative diseases caused by similar mutations, such as Huntington's disease.
This condition is rare with an estimated incidence of 1/40,000 males. Although this condition is not normally fatal eventually 20% of those affected may need a wheelchair.
Signs and symptoms
Individuals with SBMA have muscle cramps and progressive weakness due to degeneration of motor neurons in the brain stem and spinal cord. Ages of onset and severity of manifestations in affected males vary from adolescence to old age, but most commonly develop in middle adult life. The syndrome has neuromuscular and endocrine manifestations.
Neuromuscular
Early signs often include weakness of tongue and mouth muscles, fasciculations, and gradually increasing weakness of limb muscles with muscle wasting. Neuromuscular management is supportive, and the disease progresses very slowly, but can eventually lead to extreme disability. Further signs and symptoms include:
Homozygous females
Homozygous females, both of whose X chromosomes have a mutation leading to CAG expansion of the AR gene, have been reported to show only mild symptoms of muscle cramps and twitching. No endocrinopathy has been described.
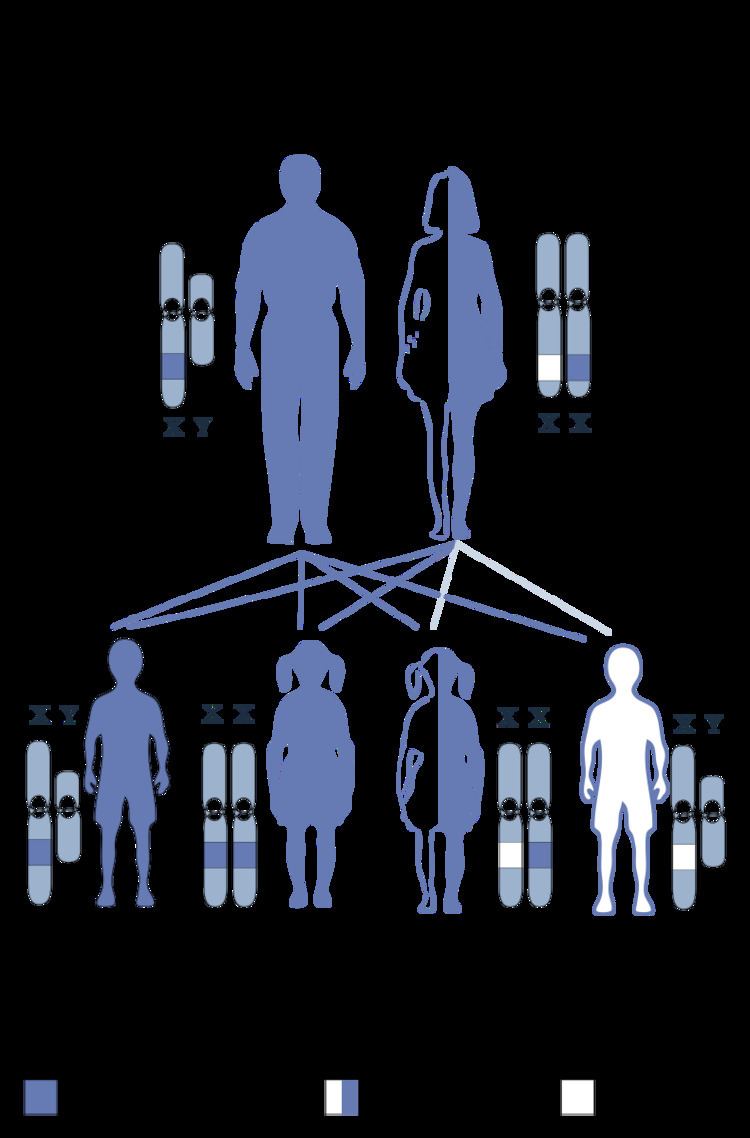
Genetics
The genetics of spinal and bulbar muscular atrophy have to do with the mutated androgen receptor gene located on the X chromosome. The effects of the mutation may be androgen-dependent, thus only males are fully affected. Females are rarely affected; female carriers tend to have a relatively mild expression of the disease if they show symptoms at all.
Pathophysiology
The mechanism behind SBMA is caused by expansion of a CAG repeat in the first exon of the androgen receptor gene (trinucleotide repeats). The CAG repeat encodes a polyglutamine tract in the androgen receptor protein. The greater the expansion of the CAG repeat, the earlier the disease onset and more severe the disease manifestations. The repeat expansion likely causes a toxic gain of function in the receptor protein, since loss of receptor function in androgen insensitivity syndrome does not cause motor neuron degeneration.
Spinal and bulbar muscular atrophy may share mechanistic features with other disorders caused by polyglutamine expansion, such as Huntington's disease. No cure for SBMA is known.
Diagnosis
In regards to the diagnosis of spinal and bulbar muscular atrophy, the AR Xq12 gene is the focus. Many mutations are reported and identified as missense/nonsense, that can be identified with 99.9% accuracy. Test for this gene in the majority of affected patients yields the diagnosis.
Management
In terms of the management of spinal and bulbar muscular atrophy, no cure is known and treatment is supportive. Rehabilitation to slow muscle weakness can prove positive, though the prognosis indicates some individuals will be wheelchair-bound in later stages of life.
Surgery may achieve correction of the spine, and early surgical intervention should be done in cases where prolonged survival is expected. Preferred nonsurgical treatment occurs due to the high rate of repeated dislocation of the hip.
Prognosis
A 2006 study followed 233 patients for a number of years. Of these, 15 died, with a median age of 65 years. The authors tentatively concluded that this is in line with a previously reported estimate of a shortened life expectancy of 10-15 years (12 in their data).
History
This disorder was first described by William R. Kennedy in 1968. In 1991, it was recognized that the AR gene is involved in the disease process. The disease is probably more common than originally thought, SBMA prevalence has been estimated at 1:50,000 males.