
 | ||
A sphygmomanometer, blood pressure meter, blood pressure monitor, or blood pressure gauge is a device used to measure blood pressure, composed of an inflatable cuff to collapse and then release the artery under the cuff in a controlled manner, and a mercury or mechanical manometer to measure the pressure. It is always used in conjunction with a means to determine at what pressure blood flow is just starting, and at what pressure it is unimpeded. Manual sphygmomanometers are used in conjunction with a stethoscope.
Contents
A sphygmomanometer consists of an inflatable cuff, a measuring unit (the mercury manometer, or aneroid gauge), and a mechanism for inflation which may be a manually operated bulb and valve or a pump operated electrically.
Types
There are three types of sphygmomanometers:
Operation
In humans, the cuff is normally placed smoothly and snugly around an upper arm, at roughly the same vertical height as the heart while the subject is seated with the arm supported. Other sites of placement depend on species, it may include the flipper or tail. It is essential that the correct size of cuff is selected for the patient. Too small a cuff results in too high a pressure, while too large a cuff results in too low a pressure. For clinical measurements it is usual to measure and record both arms in the initial consultation to determine if the pressure is significantly higher in one arm than the other. A difference of 10 mm Hg may be a sign of coarctation of the aorta. If the arms read differently, the higher reading arm would be used for later readings. The cuff is inflated until the artery is completely occluded.
With a manual instrument, listening with a stethoscope to the brachial artery at the elbow, the examiner slowly releases the pressure in the cuff. As the pressure in the cuffs falls, a "whooshing" or pounding sound is heard (see Korotkoff sounds) when blood flow first starts again in the artery. The pressure at which this sound began is noted and recorded as the systolic blood pressure. The cuff pressure is further released until the sound can no longer be heard. This is recorded as the diastolic blood pressure. In noisy environments where auscultation is impossible (such as the scenes often encountered in emergency medicine), systolic blood pressure alone may be read by releasing the pressure until a radial pulse is palpated (felt). In veterinary medicine, auscultation is rarely of use, and palpation or visualization of pulse distal to the sphygmomanometer is used to detect systolic pressure.
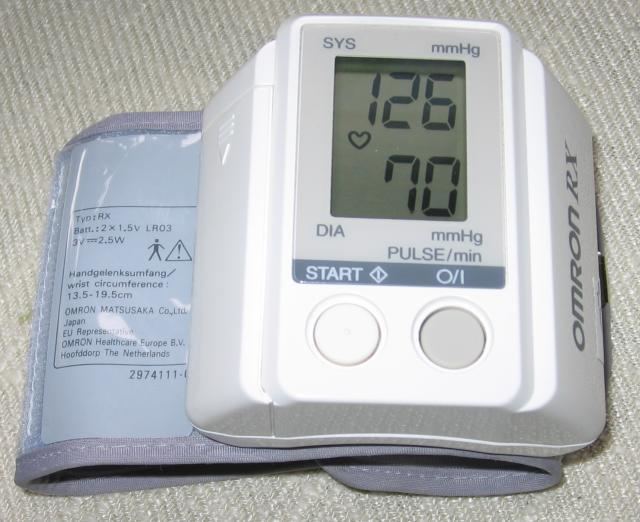
Digital instruments use a cuff which may be placed, according to the instrument, around the upper arm, wrist, or a finger, in all cases elevated to the same height as the heart. They inflate the cuff and gradually reduce the pressure in the same way as a manual meter, and measure blood pressures by the oscillometric method.
Significance
By observing the mercury in the column while releasing the air pressure with a control valve, one can read the values of the blood pressure in mm Hg. The peak pressure in the arteries during the cardiac cycle is the systolic pressure, and the lowest pressure (at the resting phase of the cardiac cycle) is the diastolic pressure. A stethoscope is used in the auscultatory method. Systolic pressure (first phase) is identified with the first of the continuous Korotkoff sounds. Diastolic pressure is identified at the moment the Korotkoff sounds disappear (fifth phase).
Measurement of the blood pressure is carried out in the diagnosis and treatment of hypertension (high blood pressure), and in many other healthcare scenarios.
Pressure sensors in digital devices
Two types of pressure sensors are typically found in digital devices: deformable membranes that are measured using differential capacitance, which is electrostatic, or differential piezoresistance.
History
The sphygmomanometer was invented by Samuel Siegfried Karl Ritter von Basch in 1881. Scipione Riva-Rocci introduced a more easily used version in 1896. In 1901, Harvey Cushing brought an example of Riva-Rocci's device to the USA, modernized it and popularized it within the medical community. Further improvement came in 1905 when Russian physician Nikolai Korotkov included diastolic blood pressure measurement following his discovery of "Korotkoff sounds."
Names
The word sphygmomanometer (/ˌsfɪɡmoʊməˈnɒmᵻtər/, SFIG-moh-mə-NOM-i-tər) uses the combining form of sphygmo- + manometer. The roots involved are as follows: Greek σφυγμός sphygmos "pulse", plus the scientific term manometer (from French manomètre), i.e. "pressure meter", itself coined from μανός manos "thin, sparse", and μέτρον metron "measure".
Most sphygmomanometers were mechanical gauges with dial faces during the first half of the 20th century. Since the advent of electronic medical devices, names such as "meter" and "monitor" can also apply, as devices can automatically monitor blood pressure on an ongoing basis.