
Pronunciation se-LE-ji-leen MedlinePlus a697046 Molar mass 187.281 g/mol | AHFS/Drugs.com Monograph License data US FDA: Selegiline CAS ID 14611-51-9 | |
 | ||
Trade names Pill form is generic and available under many brand names; transdermal patch is called Emsam Pregnancy
category AU: B2
US: C (Risk not ruled out) | ||
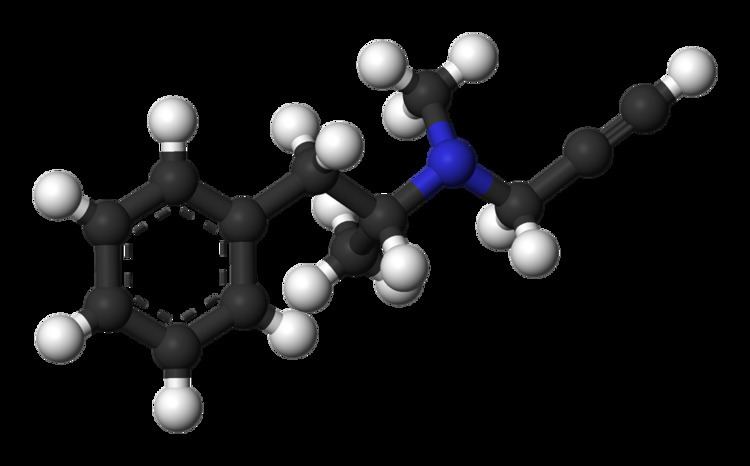
Selegiline
Selegiline, also known as -deprenyl, is a substituted phenethylamine. At normal clinical doses, it is a selective irreversible MAO-B inhibitor. In larger doses it loses its specificity and also inhibits MAO-A. It is available in pill form under many brand names and is used to reduce symptoms in early-stage Parkinson's disease. A transdermal patch (brand name, Emsam) is used to treat depression.
Contents
- Selegiline
- How to pronounce selegiline eldepryl memorizing pharmacology flashcard
- Medical uses
- Parkinsons disease
- Depression
- Veterinary use
- Adverse effects
- Interactions
- Protein binding
- Pharmacokinetics of the pill form
- Pharmacokinetics of the patch form
- Desmethylselegiline
- Levoamphetamine and levomethamphetamine
- Chemistry
- History
- Research
- Society and culture
- References
How to pronounce selegiline eldepryl memorizing pharmacology flashcard
Medical uses
For all human uses and all forms, selegiline is Pregnancy Category C, meaning that caution is in order because studies in pregnant laboratory animals have shown an adverse effect on the fetus and there are no adequate and well-controlled studies in humans, but that the drug's potential benefits may nonetheless warrant use of the drug in some pregnant women.
Parkinson's disease
In its pill form, selegiline is used to treat symptoms of Parkinson's disease. It can be used on its own or in a combination with another agent, most often L-DOPA.
Selegiline delays the time point when the L-DOPA (levodopa) treatment becomes necessary from about 11 months to about 18 months after diagnosis, which is beneficial despite not being definitive evidence of neuroprotection. The rationale for adding selegiline to levodopa is to decrease the required dose of levodopa and thus reduce the motor complications of levodopa therapy.
Depression
Selegiline is also delivered via a transdermal patch; in this form it is used as a treatment for major depressive disorder.
A quantitative review published in 2015 found that for the pooled results of the pivotal trials, the number needed to treat (a sign of effect size, so a low number is better) for the patch for symptom reduction was 11, and for remission, was 9. The number needed to harm (inverse of the NNT, a high number here is better) ranged from 387 for sexual side effects to 7 for application site reaction. With regard to the likelihood to be helped or harmed (LHH), the analysis showed that the selegiline patch was 3.6 times as likely to lead to a remission vs. a discontinuation due to side effects; the LHH for remission vs. incidence of insomnia was 2.1; the LHH for remission vs. discontinuation due to insomnia was 32.7. The LHH for remission vs insomnia and sexual dysfunction were both very low.
Veterinary use
Selegiline (brand name Anipryl) is also used (at extremely high dosages relative to humans) in veterinary medicine to treat the symptoms of Cushing's disease and cognitive dysfunction (Canine Cognitive Dysfunction) in dogs.
Adverse effects
Side effects of the pill form include, in decreasing order of frequency, nausea, hallucinations, confusion, depression, loss of balance, insomnia, increased involuntary movements, agitation, arrhythmia, slow heart rate, delusions, hypertension, new or increased angina pectoris, and syncope.
The main side effects of the patch form for depression included application site reactions, insomnia, diarrhea, and sore throat.
The selegiline transdermal patch for depression carries a black box warning about the risk of suicide, especially for young people, as do all antidepressants since 2007.
Interactions
Both forms of the drug carry strong warnings against combining selegiline with drugs that could produce serotonin syndrome, which include SSRIs and the cough medicine, dextromethorphan. Selegiline in combination with the opioid analgesic pethidine is not recommended as it can lead to severe adverse effects. Several other synthetic opioids such as tramadol and methadone, dextromethorphan, and various triptans are contraindicated due to potential for serotonin syndrome.
Both forms of the drug carry warnings about food restrictions, to avoid hypertensive crisis that are associated with MAO inhibitors. The patch form of the drug was created in part to overcome the issues with food restrictions: the clinical trials did not include food restrictions, and no hypertensive crisis during the course of them. Additionally, in post-marketing surveillance from April 2006 to October 2010, only 13 self-reports of possible hypertensive events or hypertension were made out of 29,141 exposures to the drug, and none were accompanied by objective clinical data. Nonetheless, selegiline in either form, and whether in combination with the older non-selective MAOIs or in combination with the reversible MAO-A inhibitor moclobemide, requires a low tyramine diet.
Protein binding
Selegiline is a selective inhibitor of MAO-B; MAO-B metabolizes dopamine and phenylethylamine.
Selegiline also inhibits CYP2A6 and can increase the effects of nicotine as a result. Selegiline appears to activate σ1 receptors with a relatively high affinity of approximately 400 nM.
Pharmacokinetics of the pill form
Selegiline has a low oral bioavailability, which increases to moderate when ingested together with a high-fat meal, the molecule being fat soluble.
Selegiline's oral bioavailability is drastically increased in females taking oral contraceptives (10- to 20-fold). This could lead to loss of MAO-B selectivity, with inhibition of both MAO-A and MAO-B, which would make patients susceptible to the usual risks of unselective MAOIs such as tyramine-induced hypertensive crisis and serotonin toxicity when combined with serotonergics such as SSRIs.
Pharmacokinetics of the patch form
Following application of the patch to humans, 25% to 30% of the selegiline content on average is delivered systemically over 24 hours (range approximately 10% to 40%). Transdermal dosing results in significantly higher exposure to selegiline with significantly lower exposure for all metabolites when compared to oral dosing, due to extensive first-pass metabolism for the pill form and low first-pass metabolism for the patch form. The site of application is not a significant factor in how the drug is distributed. In humans, selegiline does not accumulate in the skin nor is it metabolized in the skin.
When radiolabeled selegiline is given transdermally to laboratory animals, the drug is rapidly distributed to all body tissues and rapidly penetrates the blood–brain barrier.
Desmethylselegiline
N-Desmethylselegiline may have neuroprotective antiapoptotic properties. A large multicenter study suggests a decrease in the disease progression of Parkinsonism but may have reflected other symptomatic response. Desmethylselegiline is metabolized by CYP2C19.
Levoamphetamine and levomethamphetamine
Selegiline is partly metabolized to levomethamphetamine (L-methamphetamine), one of the two enantiomers of methamphetamine, in vivo. While these metabolites may contribute to the drug's ability to inhibit reuptake of the neurotransmitters dopamine and norepinephrine, they have also been associated with orthostatic hypotension and hallucinations in some people. A newer antiparkinson MAO-B inhibitor, rasagiline, metabolizes into 1(R)-aminoindan which has no amphetamine-like characteristics.
This metabolic pathway may cause persons taking selegiline to test positive for amphetamine or methamphetamine on drug screening tests.
Chemistry
Selegiline belongs to a class of drugs called phenethylamines. Selegiline is an L-methamphetamine derivative with a propargyl group attached to the nitrogen atom. This detail is borrowed from pargyline, an older phenethylamine MAO-B inhibitor.
Selegiline, N-methyl-N-(2-propynyl)-2-methyl-1-phenylethyl-2-amine, is synthesized by the alkylation of (–)-methamphetamine using propargyl bromide.
History
Following the discovery that the tuberculosis (TB) drug iproniazid elevated the mood of people taking it for TB, and the subsequent discovery that the effect was likely due to inhibition of MAO, many people and companies started trying to discover MAO inhibitors to use as antidepressants. Selegiline was discovered by Z. Ecseri at the Hungarian drug company, Chinoin (part of Sanofi since 1993), which they called E-250. Chinoin received a patent on the drug in 1962 and the compound was first published in the scientific literature in English in 1965. Work on the biology and effects of E-250 in animals and humans was conducted by a group led by József Knoll at Semmelweis University which was also in Budapest.
Deprenyl is a racemic compound, a mixture of two isomers called enantiomers. Further work determined that the levorotatory enantiomer was a more potent MAO-inhibitor, which was published in 1967, and subsequent work was done with the single enantiomer L-deprenyl.
In 1971, Knoll showed that selegiline selectively inhibits the B-isoform of monoamine oxidase (MAO-B) and proposed that it is unlikely to cause the infamous "cheese effect" (hypertensive crisis resulting from consuming foods containing tyramine) that occurs with non-selective MAO inhibitors. A few years later, two Parkinson's disease researchers based in Vienna, Peter Riederer and Walther Birkmayer, realized that selegiline could be useful in Parkinson's disease. One of their colleagues, Prof. Moussa B.H. Youdim, visited Knoll in Budapest and took selegiline from him to Vienna. In 1975, Birkmayer's group published the first paper on the effect of selegiline in Parkinson's disease.
The discovery that selegiline seemed to have a neuroprotection effect in Parkinson's disease led to widespread speculation in the 1970s that it could be useful as an anti-aging drug.
In 1987 Somerset Pharmaceuticals in New Jersey, which had acquired the US rights to develop selegiline, filed a new drug application (NDA) with the FDA to market the drug for PD in the US. While the NDA was under review, Somerset was acquired in a joint venture by two generic drug companies, Mylan and Bolan Pharmaceuticals. Selegiline was approved for Parkinson's disease by the FDA in 1989.
In the 1990s, J. Alexander Bodkin at McLean Hospital, an affiliate of Harvard Medical School, began a collaboration with Somerset to develop delivery of selegiline via a transdermal patch in order to avoid the well known dietary restrictions of MAO inhibitors. Somerset obtained FDA approval to market the patch in 2006.
Research
A selegiline transdermal patch was tested for its effectiveness in treating ADHD.
Selegiline's effectiveness in helping people stop smoking tobacco or cannabis has been studied.
Society and culture
Due to the structural similarity to amphetamine, selegiline has been classified as a controlled substance in Japan and thus can only be obtained with a prescription or special government license. Amphetamine and methamphetamine are illegal in the country.
In E for Ecstasy (a book examining the uses of the street drug ecstasy in the UK) the writer, activist and ecstasy advocate Nicholas Saunders highlighted test results showing that certain consignments of the drug also contained selegiline. Consignments of ecstasy known as "Strawberry" contained what Saunders described as a "potentially dangerous combination of ketamine, ephedrine and selegiline," as did a consignment of "Sitting Duck" Ecstasy tablets.
In the US, selegiline is available by prescription but is not scheduled as a controlled substance.