
Specialty endocrinology ICD-9-CM 260-263 MeSH D011502 | ICD-10 E40-E44 eMedicine derm/797 | |
 | ||
Protein–energy malnutrition (PEM) or protein–calorie malnutrition refers to a form of malnutrition where there is inadequate calorie or protein intake.
Contents
Types include:
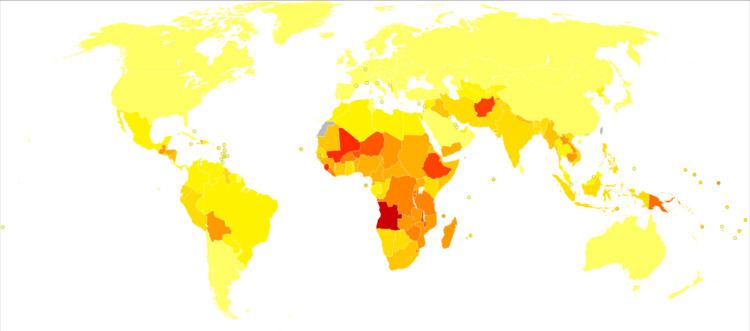
PEM is fairly common worldwide in both children and adults and accounts for 6 million deaths annually. In the industrialized world, PEM is predominantly seen in hospitals, is associated with disease, or is often found in the elderly.
Note that PEM may be secondary to other conditions such as chronic renal disease or cancer cachexia in which protein energy wasting may occur.
Protein–energy malnutrition affects children the most because they have less protein intake. The few rare cases found in the developed world are almost entirely found in small children as a result of fad diets, or ignorance of the nutritional needs of children, particularly in cases of milk allergy.
Prenatal protein malnutrition
Protein malnutrition is detrimental at any point in life, but protein malnutrition prenatally has been shown to have significant lifelong effects. During pregnancy, one should aim for a diet that consists of at least 20% protein for the health of the fetus. Diets that consist of less than 6% protein in utero have been linked with many deficits, including decreased brain weight, increased obesity, and impaired communication within the brain in some animals. Even diets of mild protein malnutrition (7.2%) have been shown to have lasting and significant effects in rats. The following are some studies in which prenatal protein deficiency has been shown to have unfavorable consequences.
From these studies it is possible to conclude that prenatal protein nutrition is vital to the development of the fetus, especially the brain, the susceptibility to diseases in adulthood, and even gene expression. When pregnant females of various species were given low-protein diets, the offspring were shown to have many deficits. These findings highlight the great significance of adequate protein in the prenatal diet.
Epidemiology
Although protein energy malnutrition is more common in low-income countries, children from higher-income countries are also affected, including children from large urban areas in low socioeconomic neighborhoods. This may also occur in children with chronic diseases, and children who are institutionalized or hospitalized for a different diagnosis. Risk factors include a primary diagnosis of intellectual disability, cystic fibrosis, malignancy, cardiovascular disease, end stage renal disease, oncologic disease, genetic disease, neurological disease, multiple diagnoses, or prolonged hospitalization. In these conditions, the challenging nutritional management may get overlooked and underestimated, resulting in an impairment of the chances for recovery and the worsening of the situation.
PEM is fairly common worldwide in both children and adults and accounts for 6 million deaths annually. In the industrialized world, PEM is predominantly seen in hospitals, is associated with disease, or is often found in the elderly.
Co-morbidity
A large percentage of children that suffer from PEM also have other co-morbid conditions. The most common co-morbidities are diarrhea (72.2% of a sample of 66 subjects) and malaria (43.3%). However, a variety of other conditions have been observed with PEM, including sepsis, severe anaemia, bronchopneumonia, HIV, tuberculosis, scabies, chronic suppurative otitis media, rickets, and keratomalacia. These co-morbidities tax already malnourished children and may prolong hospital stays initially for PEM and may increase the likelihood of death.