
 Similar Prostatic acid phosphatase, Prostate specific antigen, Prostate cancer screening | ||
Prostate cancer staging is the process by which physicians categorize the risk of cancer having spread beyond the prostate, or equivalently, the probability of being cured with local therapies such as surgery or radiation. Once patients are placed in prognostic categories, this information can contribute to the selection of an optimal approach to treatment. The information considered in such a prognostic classification can be based on physical examination, imaging studies and blood tests (so-called "clinical stage"), or based on the extent of disease as revealed in a surgical specimen (so-called "pathologic stage").
Contents
- TNM staging
- Evaluation of the primary tumor T
- Evaluation of the regional lymph nodes N
- Evaluation of distant metastasis M
- Evaluation of the histologic grade G
- Overall staging
- Whitmore Jewett staging
- Risk groups
- References
There are two schemes commonly used to stage Prostate cancer. The most common is promulgated by the American Joint Committee on Cancer, and is known as the TNM system, which evaluates the size of the tumor, the extent of involved lymph nodes, and any metastasis (distant spread) and also takes into account cancer grade. As with many other cancers, these are often grouped into four stages (I–IV). Another scheme, now used less commonly for research, but often still used by clinicians, is the Whitmore-Jewett stage.
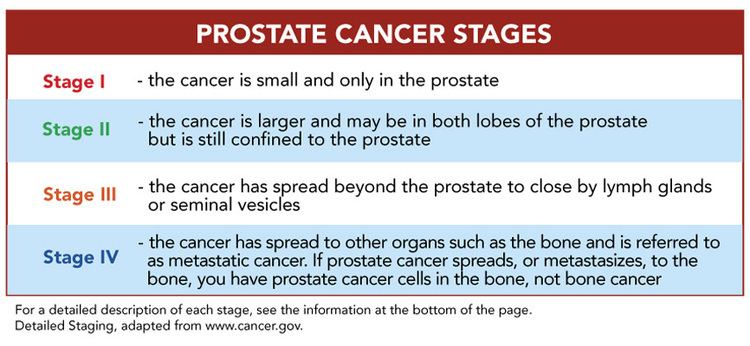
Briefly, Stage I disease is cancer that is found incidentally in a small part of the sample when prostate tissue was removed for other reasons, such as benign prostatic hypertrophy, and the cells closely resemble normal cells and the gland feels normal to the examining finger. In Stage II more of the prostate is involved and a lump can be felt within the gland. In Stage III, the tumor has spread through the prostatic capsule and the lump can be felt on the surface of the gland. In Stage IV disease, the tumor has invaded nearby structures, or has spread to lymph nodes or other organs. The Gleason grading system is based on cellular content and tissue architecture from biopsies, which provides an estimate of the destructive potential and ultimate prognosis of the disease.
TNM staging
From the AJCC 6th edition (2002) and UICC 6th edition.
Evaluation of the (primary) tumor ('T')
It should be stressed that the designation "T2c" implies a tumor which is palpable in both lobes of the prostate. Tumors which are found to be bilateral on biopsy only but which are not palpable bilaterally should not be staged as T2c.
Evaluation of the regional lymph nodes ('N')
Evaluation of distant metastasis ('M')
Evaluation of the histologic grade ('G')
Usually, the grade of the cancer (how different the tissue is from normal tissue) is evaluated separately from the stage; however, for prostate cancer, grade information is used in conjunction with TNM status to group cases into four overall stages.
Of note, this system of describing tumors as "well-", "moderately-", and "poorly-" differentiated based on Gleason score of 2-4, 5-6, and 7-10, respectively, persists in SEER and other databases but is generally outdated. In recent years pathologists rarely assign a tumor a grade less than 3, particularly in biopsy tissue. A more contemporary consideration of Gleason grade is:
Note that under current guidelines, if any Pattern 5 is present it is included in final score, regardless of the percentage of the tissue having this pattern, as the presence of any pattern 5 is considered to be a poor prognostic marker.
Overall staging
The tumor, lymph node, metastasis, and grade status can be combined into four stages of worsening severity.
Whitmore-Jewett staging
The Whitmore-Jewett system is similar to the TNM system, with approximately equivalent stages. Roman numerals are sometimes used instead of Latin letters for the overall stages (for example, Stage I for Stage A, Stage II for Stage B, and so on).
Risk groups
While TNM staging is important, systems based just on anatomic features are not well suited for deciding what treatment is best for a patient with prostate cancer, as there is still considerable heterogeneity of prognosis within the stage categories. A more refined prognosis can be established by consideration of prostate specific antigen, and grade (i.e. Gleason score in the Gleason grading system ). For example, it is now common to classify patients into high, intermediate and low risk groups on the basis of these three factors (TNM stage, PSA and Gleason score). Currently, there is no clear division between stage, which is historically a statement of anatomic extent of disease at diagnosis, and prognostic models that may include many features that contribute to clinical outcome.
If treated, patients with low risk disease are usually treated with active surveillance, prostatectomy, or radiotherapy alone. Patients with intermediate risk disease are candidates for prostatectomy or radiotherapy and a short duration (less than 6 months) of hormonal ablation (medical castration using a gonadotropin-releasing hormone analog). Although the role of surgery in these patients remains uncertain, those with high risk disease are usually treated with radiotherapy and a long duration of hormonal ablation. Many high risk patients are not cured by this treatment, and the search for better treatments in this group is a particularly pressing concern in prostate cancer research.