
 | ||
Prolonged grief disorder (PGD) refers to a syndrome consisting of a distinct set of symptoms following the death of a loved one. PGD is relatively rare – experienced by about 10 percent of bereaved survivors, though rates vary depending on the circumstances. The affected person is incapacitated by grief, so focused on the loss that it is difficult to care about much else. He or she often ruminates about the death and longs for a reunion with the departed, while feeling unsure of his or her own identity and place in the world. The victim will develop a flat and dull outlook on life, feeling that the future holds no prospect of joy, satisfaction or pleasure. The bereaved person who suffers from PGD feels devalued and in constant turmoil, with an inability to adjust to (if not a frank protest against) life without the beloved.
Contents
- Description
- History and discussion
- Difference from normal grief
- Diagnostic criteria
- Risk factors
- Health consequences
- Treatment
- Incidence
- References
PGD is defined by its symptoms, duration and intensity. The symptoms are intense yearning for the person, identity confusion, difficulty accepting the loss, bitterness, emotional numbness, inability to trust others and the feeling of being trapped in grief. These are present every day, causing significant distress and functional impairment, and remaining intense, frequent, and disabling for six months or more after the death.
Description
Grief is a normal response to bereavement. Researchers have found that 10–20% of people experience a prolonged response to bereavement that impacts functioning and has adverse long-term effects on health.
Prolonged grief is considered when an individual's ability to function and level of distress over the loss is extreme and persistent. People with PGD feel "stuck" in their grief, experience a chronic aching and yearning for the dear departed, feel that they are not the same person anymore (e.g., unsure of their identity, loss of a sense of self and self-worth), become emotionally disconnected from others, and lack the desire to "move on" (sometimes feeling that doing so would be betraying the person who is now deceased).
History and discussion
The DSM-IV and ICD-10 do not distinguish between normal and prolonged grief. Based on numerous findings of maladaptive effects of prolonged grief, diagnostic criteria for PGD have been proposed for inclusion in the DSM-5 and ICD-11.
The proposed diagnostic criteria were the result of statistical analysis of a set of criteria agreed upon by a panel of experts. The analyses produced criteria that were the most accurate markers of bereaved individuals suffering from painful, persistent, destructive PGD. The criteria for PGD have been validated and dozens of studies both internationally and domestically are being conducted, and published, that validate the PGD criteria in other cultures, kinship relationships to the deceased and causes of death (e.g., earthquakes, tsunami, war, genocide, fires, bombings, palliative and acute care settings).
Recognizing prolonged grief as a disorder would allow it to be better understood, detected, studied and treated. Insurance companies would also be more likely reimburse its care. On the other hand, inclusion of PGD in the DSM-5 and ICD-11 may be misunderstood as the medicalization of grief, reducing its dignity, turning love into pathology and implying that survivors should quickly forget and "get over" the loss. Bereaved persons may be insulted by having their distress labeled as a mental disorder. While this stigmatization would not be the intent, it might be an unintended consequence. In spite of this concern, studies have shown that nearly all bereaved individuals who met the criteria for PGD were receptive to treatment and their families relieved to know they had a recognizable syndrome.
Difference from normal grief
Although extremely painful, grief is the normal process of accommodating to a new life without the deceased loved one. Most bereaved survivors manage to get through the worst of their grief and continue to function and find meaning in life. Normal grief differs from PGD in that it is not as intense, persistent, disabling and life-altering and is not experienced as a severe threat to the survivor's identity, sense of self-worth, feeling of security, safety or hopes for future happiness. Although normal grief remains with the bereaved person far into the future, its ability to disrupt the survivor's life dissipates with time.
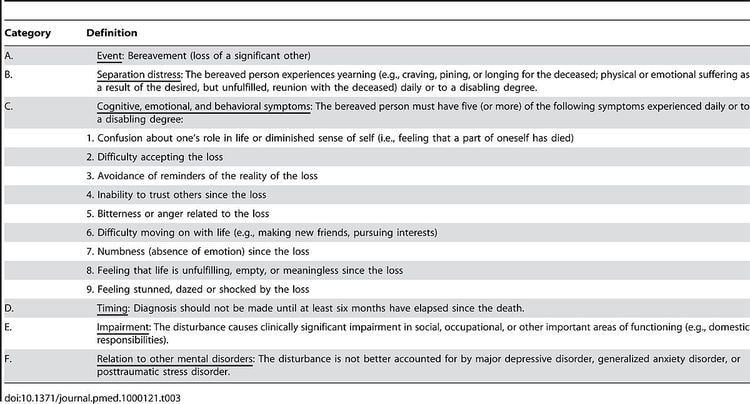
Diagnostic criteria
Factor analytic studies have determined that the symptoms of PGD form a unitary construct that is separate from symptoms of bereavement-related depression and anxiety. Extensive research has been conducted to identify and isolate the symptoms that constitute PGD and distinguish it from diagnostic "nearest neighbors" such as Major Depressive Disorder or Posttraumatic Stress Disorder. These analyses integrate clinical insights with rigorous empirical analysis to determine the set of symptoms that best indicate which bereaved survivors will be at risk of long term dysfunction and distress (e.g., suicidality, alcohol abuse, disability days, sleep impairment, quality of life impairment, high blood pressure, hospitalizations for serious medical events such as heart attacks).
Prigerson et al. proposed diagnostic criteria for PGD for inclusion in the DSM-5 and ICD-11.
Risk factors
Known risk factors and clinical correlates for PGD include a history of:
These risk factors and clinical correlates have been shown to relate to PGD symptoms and not symptoms of Major Depressive Disorder (MDD), Post-traumatic Stress Disorder (PTSD), and Generalized Anxiety Disorder (GAD).
Health consequences
PGD symptoms have been associated with:
Treatment
The unique symptom profile and course of PGD requires targeted treatment. Randomized control trials (RCT) have proven tricyclic antidepressants alone or together with interpersonal psychotherapy ineffective in reducing PGD symptoms, while psychotherapy designed specifically for PGD has been proven to be beneficial. Preliminary results of an online, self-management intervention to prevent PGD in recently bereaved individuals, in a study called "HEAL" (Healthy Experiences After Loss), are very promising. A larger randomized controlled trial is being planned.
Incidence
Out of the people surveyed who have experienced a loss, 10–20% display a prolonged and severe grief response. Global incidence needs further investigation.