
ICD-10 C90.1 ICD-O M9733/3 | ICD-9-CM 203.1 MeSH D007952 | |
 | ||
Specialty Hematology and oncology | ||
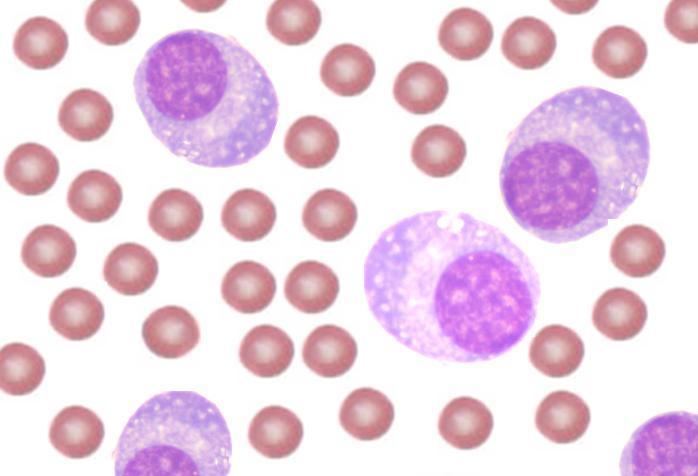
Plasma cell leukemia (PCL), a lymphoproliferative disorder, is a rare cancer involving a subtype of white blood cells called plasma cells. Plasma cell leukemia is one of the most aggressive human neoplasms and constitutes 2% to 4% of all cases of plasma cell disorders. The WHO criterion for diagnosis of PCL is that plasma cells constitute more than 20% of cells in the peripheral blood with an absolute plasma cell count of more than 2 × 109/L. The presentation may be primary, de novo, or secondary, evolving from an existing case of multiple myeloma as part of the terminal phase of the disease. Approximately 60 to 70% of cases are primary.
Contents
Laboratory findings
Although there is overlap, the markers of plasma cells from patients with primary PCL is different from those of myeloma patients. PCL plasma cells more frequently express the CD20 antigen than those of multiple myeloma (50% vs. 17%), and they often lack CD56 antigen which is present on the majority of myeloma cells. CD56 is considered important in anchoring plasma cells to bone marrow stroma, and its expression is associated with a poor prognosis. CD28 is more frequently expressed on malignant plasma cells in secondary than in primary PCL, which is consistent with an observation made in myeloma, that is, that acquisition of the CD28 antigen on plasma cells appears to correlate with an increased proliferative rate and disease progression.
The chromosome characteristics or karyotypes of PCL plasma cells is complex. Using fluorescence in situ hybridization techniques, losses in the long arm of chromosome 13 (13q) and deletion of one the homologous chromosomes 13 (monosmy 13) exist in more than 80% of PCL patients. Losses on chromosome 16 also occur in approximately 80% of cases. Gains in long arm of chromosome 1 (1q) are present in approximately one-half of the patients determined by FISH, but in all patients by comparative genomic hybridization. Overexpression of the protein PRAD1/cyclin D1, which plays an important role in control of the cell cycle, has also been observed in PCL. Plasma cell leukemia is more frequent in light-chain (Bence Jones protein) or IgD myeloma. It is seen less frequently in IgA or IgG myeloma (see: multiple myeloma).
Clinical course
The clinical presentation of primary PCL is more aggressive than that of multiple myeloma, and the clinical features found in PCL involves combination of those found in acute leukemia and those found in myeloma. PCL patients have a higher presenting tumor burden; higher frequencies of (involvement of organs other than the bone marrow by disease), thrombocytopenia (decreased platelet count), anemia, hypercalcemia (elevated blood calcium), and renal impairment; increased levels of serum lactate dehydrogenase (LDH) and β-2 macroglobulin and plasma cell proliferative activity. The incidence of lytic bone lesions is slightly lower than that usually observed in multiple myeloma. PCL is extremely aggressive associated with short survival (median survival of 6–8 months).
Therapy and prognosis
Treatment of plasma cell leukemia is by supportive care and systemic chemotherapy. Combination of cyclophosphamide, doxorubicin, vincristine, and prednisone (or dexamethasone) can be used. A second combination is the use of cyclophosphamide, dexamethasone, and thalidomide as for myeloma. Another regimen termed VMCP/VBAP uses alternating vincristine, melphalan (M), cyclophosphamide, prednisone/vincristine, carmustine, doxorubicin, and prednisone polychemotherapy. In general, combination chemotherapy has resulted in median survivals of 18 to 20 months compared to 2 to 6 months when single agent therapy is used. There are anecdotal reports of excellent responses and 2- to 3-year disease-free survivals after autologous stem cell transplantation. Autologous transplantation may increase benefit from conventional therapy and high dose melphalan may prolong progression free and overall survival.
Although the clinical and laboratory features of primary and secondary PCL are similar, the response to therapy and overall survival in primary and secondary PCL go from poor to worse. Patients with secondary PCL are usually refractory to chemotherapy and have a poor survival compared with duration (median <2 months).
Novel agents like thalidomide, lenalidomide and bortezomib have been recently used, alone or in combination with conventional chemotherapeutics like melphalan or cyclophosphamide. Two cases had encouraging results with bortezomib. Recent studies demonstrate that velcade (bortezomib)- based regimens offer a significant profit in patients suffering from PCL. More aggressive therapeutic regimens like DT-PACE or protocols used in ALL offer a significant response rate, but with short remission interval.