
Precursor dental follicle FMA 56665 | Latin fibra periodontalis | |
 | ||
The periodontal ligament, commonly abbreviated as the PDL, is a group of specialized connective tissue fibers that essentially attach a tooth to the alveolar bone within which it sits.
Contents
Development
Similar to the alveolar bone, the PDL develops from the dental sac of the tooth germ.
Features
Functions of PDL are supportive, sensory, nutritive, and remodeling.
The PDL substance has been estimated to be 70% water, which is thought to have a significant effect on the tooth's ability to withstand stress loads. The completeness and vitality of the PDL are essential for the functioning of the tooth.
The PDL ranges in width from 0.15 to 0.38mm with its thinnest part located in the middle third of the root.
The PDL is a part of the periodontium that provide for the attachment of the teeth to the surrounding alveolar bone by way of the cementum.
The PDL appears as the periodontal space of 0.4 to 1.5 mm on radiographs, a radiolucent area between the radiopaque lamina dura of the alveolar bone proper and the radiopaque cementum.
There are progenitor cells in the periodontal ligament that can differentiate into osteoblasts for the physiological maintenance of alveolar bone and, most likely, for its repair as well.
Structure
The PDL consist of cells, and extracellular compartment of fibers. The cells are fibroblast, epithelial cells, undifferentiated mesenchymal cells, bone and cementum cells. The epithelial rests of Malassez are also present; these groups of epithelial cells become located in the mature PDL after the disintegration of Hertwig epithelial root sheath during the formation of the root. The extracellular compartment consists of Type 1, 3, and 5 collagen fibers bundles embedded in intercellular substance. The PDL collagen fibers are categorized according to their orientation and location along the tooth.
Alveolodental ligament
The main principal fiber group is the alveolodental ligament, which consists of five fiber subgroups: alveolar crest, horizontal, oblique, apical, and interradicular on multirooted teeth. Principal fibers other than the alveolodental ligament are the transseptal fibers.
All these fibers help the tooth withstand the naturally substantial compressive forces which occur during chewing and remain embedded in the bone. The ends of the principal fibers that are within either cementum or alveolar bone proper are considered Sharpey fibers.
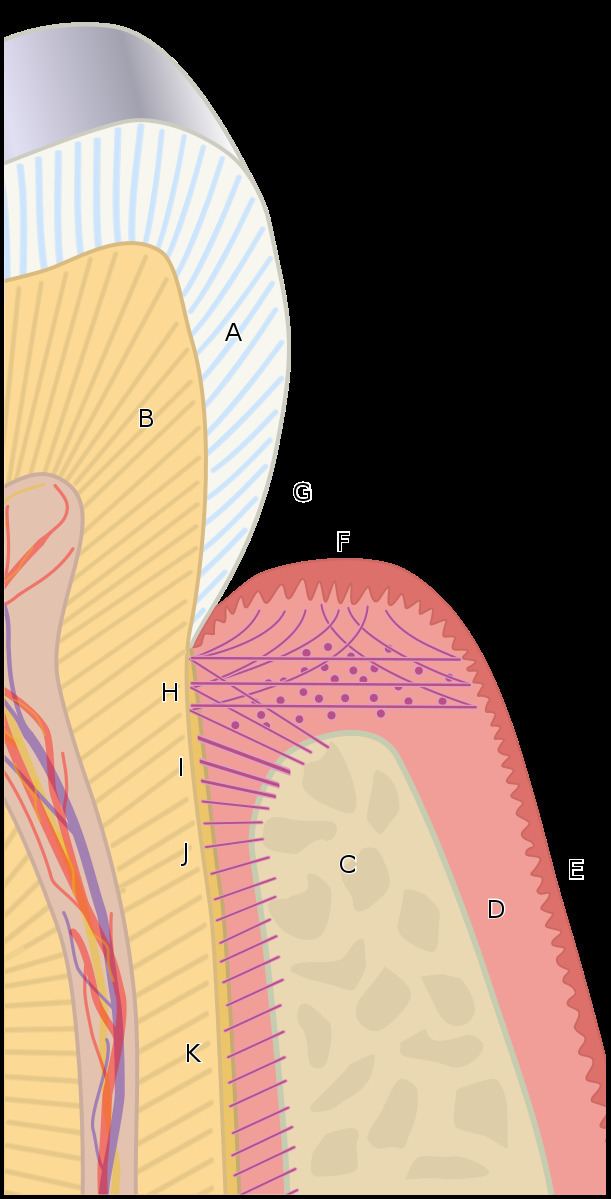
Alveolar crest fibers
Alveolar crest fibers (I)run from the cervical part of the root to the alveolar bone crest
Horizontal fibers
Horizontal fibers (J) attach to the cementum apical to the alveolar crest fibers and run perpendicularly from the root of the tooth to the alveolar bone.
Oblique fibers
Oblique fibers (K) are the most numerous fibers in the periodontal ligament, running from cementum in an oblique direction to insert into bone coronally.
Apical fibers
Apical fibers are found radiating from cementum around the apex of the root to the bone, forming base of the socket or alveolus.
Interradicular fibers
Interradicular fibers are only found between the roots of multirooted teeth, such as premolars and molars. They extend from radicular cementum to interradicular alveolar bone.
Transseptal fibers
Transseptal fibers (H) extend interproximally over the alveolar bone crest and are embedded in the cementum of adjacent teeth; they form an interdental ligament. These fibers keep all the teeth aligned. These fibers may be considered as belonging to the gingival tissue because they do not have an osseous attachment.