
ICD-10 O70.0—O70.3, O71.8 | ||
 | ||
Synonym Latin: Laceratio perinei | ||
In obstetrics, a perineal tear is a spontaneous (unintended) laceration of the skin and other soft tissue structures which, in women, separate the vagina from the anus. Perineal tears mainly occur in women as a result of vaginal childbirth, which strains the perineum. Tears vary widely in severity. The majority are superficial and require no treatment, but severe tears can cause significant bleeding, long-term pain or dysfunction. A perineal tear is distinct from an episiotomy, in which the perineum is intentionally incised to facilitate delivery.
Contents
Anatomy
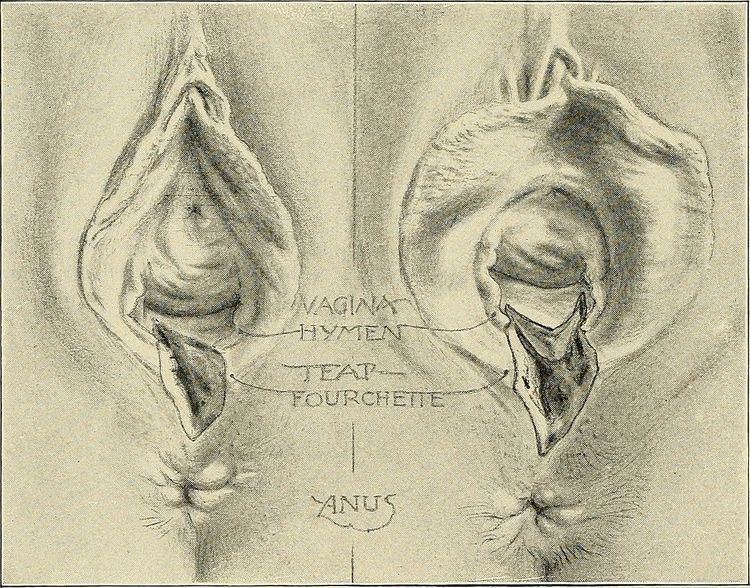
In a woman, an anatomical area known as the perineum separates the opening of the vagina from that of the anus. Each opening is surrounded by a wall, and the anal wall is separated from the vaginal wall by a mass of soft tissue including:
A perineal tear may involve some or all of these structures, which normally aid in supporting the pelvic organs and maintaining faecal continence.
Classification
Tears are classified into four categories:
Cause
In humans and some other primates, the head of the term fetus is so large in comparison to the size of the birth canal that term delivery is rarely possible without some degree of trauma. As the head passes through the pelvis, the soft tissues are stretched and compressed. The risk of severe tear is greatly increased if the fetal head is oriented occiput posterior (face forward), if the mother has not given birth before or if the fetus is large.
Prevention
Several techniques are used to reduce the risk of tearing, but with little evidence for efficacy. Antenatal digital perineal massage is often advocated, and may reduce the risk of trauma only in nulliparous women. ‘Hands on’ techniques employed by midwives, in which the foetal head is guided through the vagina at a controlled rate have been widely advocated, but their efficacy is unclear. Waterbirth and labouring in water are popular for several reasons, and it has been suggested that by softening the perineum they might reduce the rate of tearing. However, this effect has never been clearly demonstrated.
Prevalence
A 2008 study found that over 85% of women having a vaginal birth sustain some form of perineal trauma, and 60-70% receive stitches. A retrospective study of 8,603 vaginal deliveries in 1994 found a third degree tear had been clinically diagnosed in only 50 women (0.6%). However, when the same authors used anal endosonography in a consecutive group of 202 deliveries, there was evidence of third degree tears in 35% of first-time mothers and 44% of mothers with previous children. These numbers are confirmed by other researchers in 1999.
Complications
First and second degree tears rarely cause long-term problems. Among women who experience a third or fourth degree tear, 60-80% are asymptomatic after 12 months. Faecal incontinence, faecal urgency, chronic perineal pain and dyspareunia occur in a minority of patients, but may be permanent. The symptoms associated with perineal tear are not always due to the tear itself, since there are often other injuries, such as avulsion of pelvic floor muscles, that are not evident on examination.
Insurance Coverage
A study by the Agency for Healthcare Research and Quality (AHRQ) found that in 2011, first- and second-degree perineal tear was the most common complicating condition for vaginal deliveries in the U.S. among women covered by either private insurance or Medicaid. Second-degree perineal laceration rates were higher for women covered by private insurance than for women covered by Medicaid.