
Specialty endocrinology OMIM 274600 GeneReviews Pendred Syndrome/DFNB4 | ICD-10 E07.1 DiseasesDB 9771 | |
 | ||
Pendred syndrome or Pendred disease is a genetic disorder leading to congenital bilateral (both sides) sensorineural hearing loss and goitre with euthyroid or mild hypothyroidism (decreased thyroid gland function). There is no specific treatment, other than supportive measures for the hearing loss and thyroid hormone supplementation in case of hypothyroidism. It is named after Dr Vaughan Pendred (1869–1946), the English doctor who first described the condition in an Irish family living in Durham in 1896. It accounts for 7.5% of all cases of congenital deafness.
Contents
Signs and symptoms
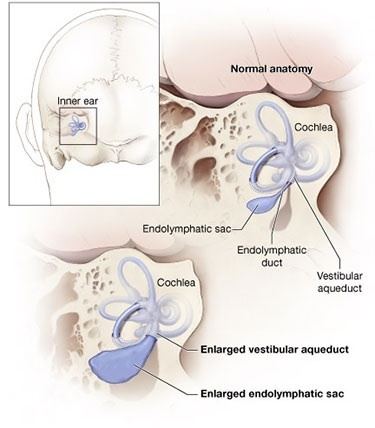
The hearing loss of Pendred's syndrome is often, although not always, present from birth, and language acquisition may be a significant problem if deafness is severe in childhood. The hearing loss typically worsens over the years, and progression can be step-wise and related to minor head trauma. In some cases, language development worsens after head injury, demonstrating that the inner ear is sensitive to trauma in Pendred syndrome; this is as a consequence of the widened vestibular aqueducts usual in this syndrome. Vestibular function varies in Pendred syndrome and vertigo can be a feature of minor head trauma. A goitre is present in 75% of all cases.
Genetics
Pendred syndrome inherits in an autosomal recessive manner, meaning that one would need to inherit an abnormal gene from each parent to develop the condition. This also means that a sibling of a patient with Pendred's syndrome has a 25% chance of also having the condition if the parents are unaffected carriers.
It has been linked to mutations in the PDS gene, which codes for the pendrin protein (solute carrier family 26, member 4, SLC26A4). The gene is located on the long arm of chromosome 7 (7q31). Mutations in the same gene also cause enlarged vestibular aqueduct syndrome (EVA or EVAS), another congenital cause of deafness; specific mutations are more likely to cause EVAS, while others are more linked with Pendred syndrome.
Pathophysiology
SLC26A4 can be found in the cochlea (part of the inner ear), thyroid and the kidney. In the kidney, it participates in the secretion of bicarbonate. However, Pendred's syndrome is not known to lead to kidney problems. It functions as an iodide/chloride transporter. In the thyroid, this leads to reduced organification of iodine (i.e. its incorporation into thyroid hormone).
Diagnosis
Audiometry (measuring ability to hear sounds of a particular pitch) is usually abnormal, but the findings are not particularly specific and an audiogram is not sufficient to diagnose Pendred's syndrome. A thyroid goitre may be present in the first decade and is usual towards the end of the second decade. MRI scanning of the inner ear usually shows widened or large vestibular aqueducts with enlarged endolymphatic sacs and may show abnormalities of the cochleae that is known as Mondini dysplasia. Genetic testing to identify the pendrin gene usually establishes the diagnosis. If the condition is suspected, a "perchlorate discharge test" is sometimes performed. This test is highly sensitive, but may also be abnormal in other thyroid conditions. If a goitre is present, thyroid function tests are performed to identify mild cases of thyroid dysfunction even if they are not yet causing symptoms.
Treatment
No specific treatment exists for Pendred syndrome. Speech and language support and cochlear implants may improve language skills. If thyroid hormone levels are decreased, thyroid hormone supplements may be required. Patients are advised to take precautions against head injury.