
 | ||
Patient derived tumor xenograft pdx
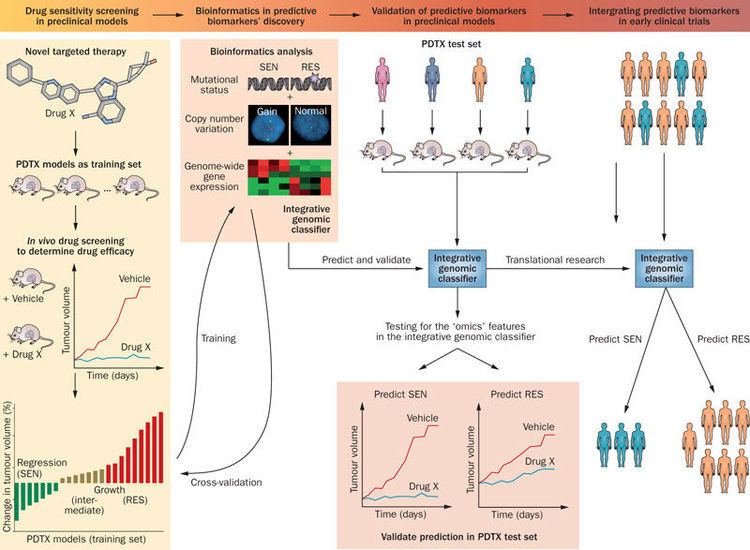
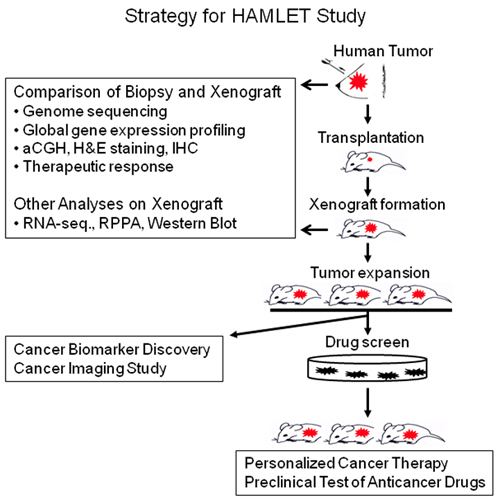
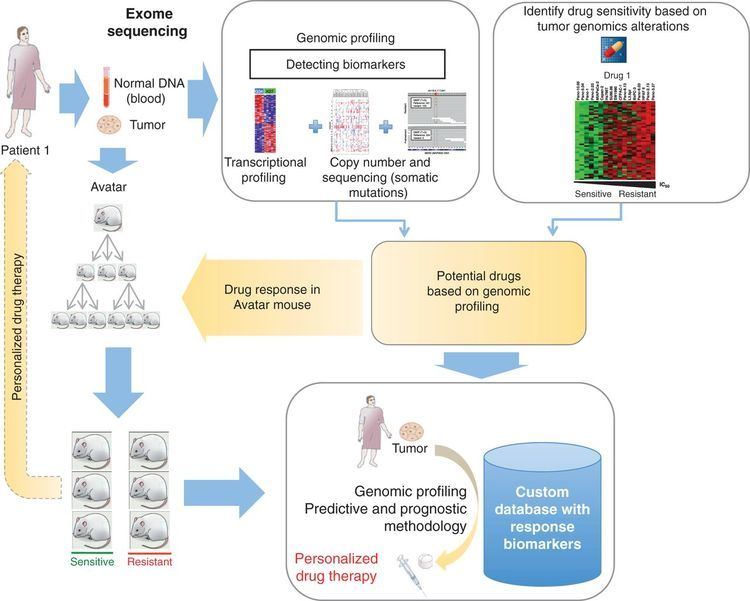
Patient derived tumor xenografts (PDTX) are created when cancerous tissue from a patient’s primary tumor is implanted directly into an immunodeficient mouse. PDTX models are providing solutions to the challenges that researchers face in cancer drug research such as positive tumor responses in mouse models but not translating over when the study is implemented in humans. As a result, PDTX cancer models are becoming popular models to use in cancer drug research.
Contents
- Patient derived tumor xenograft pdx
- Methods of tumor xenotransplantation
- Advantages over cancer cell lines
- Humanized xenograft models
- Breast cancer
- Colorectal cancer
- Pancreatic cancer
- Pediatric cancer neuroblastoma
- Challenges with PDTX model adaptation
- References
Methods of tumor xenotransplantation
Several types of immunodeficient mice can be used to establish PDTX models: athymic nude mice, severely compromised immune deficient (SCID) mice, nonobese diabetic (NOD)-SCID mice, and recombination-activating gene 2 (Rag2)-knockout mice. The mice used must be immunocompromised to prevent transplant rejection. The NOD-SCID mouse is considered more immunodeficient than the nude mouse, and therefore is more commonly used for PDTX models because the NOD-SCID mouse does not produce Natural Killer cells.
When human tumors are resected, necrotic tissues are removed and the tumor can be mechanically sectioned into smaller fragments, chemically digested, or physically manipulated into a single-cell suspension. There are advantages and disadvantages in utilizing either discrete tumor fragments or single-cell suspensions. Tumor fragments retain cell-cell interactions as well as some tissue architecture of the original tumor, therefore mimicking the tumor microenvironment. Alternatively, a single-cell suspension enables scientists to collect an unbiased sampling of the whole tumor, eliminating spatially segregate subclones that are otherwise inadvertently selected during analysis or tumor passaging However, single-cell suspensions subject surviving cells to harsh chemical or mechanical forces that may sensitize cells to anoikis, taking a toll on cell viability and engraftment success.
Unlike creating xenograft mouse models using existing cancer cell lines, there are no intermediate in vitro processing steps before implanting tumor fragments murine host to create a PDTX. The tumor fragments are either be implanted heterotopically or orthotopically of an immunodeficient mouse. Heterotopical implants occur when the tumor fragment is implanted into an area of the mouse unrelated to the original tumor site, generally subcutaneously or subrenal capsular sites. Whereas, scientists tranplant the patient’s tumor tissue and implants the fragments into the corresponding anatomical position in the mouse in an orthotopic transplant. Subcutaneous PDTX rarely produce metastasis in mice, does not simulate the initial tumor microenvironment, and has engraftment rates 40-60%. Subrenal capsular PDTX maintains the original tumor stroma as well as the equivalent host stroma and has an engraftment rate of 95%. Ultimately, the time it takes about 2 to 4 months for the tumor to engraft varying by tumor type, implant location, and strain of immunodeficient mice utilized; engraftment failure should not be declared until at least 6 months.
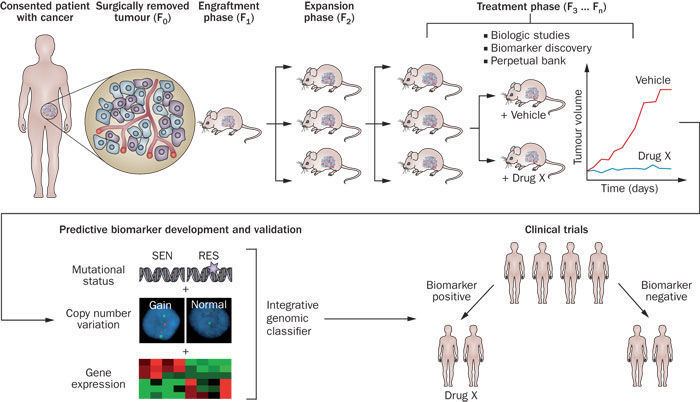
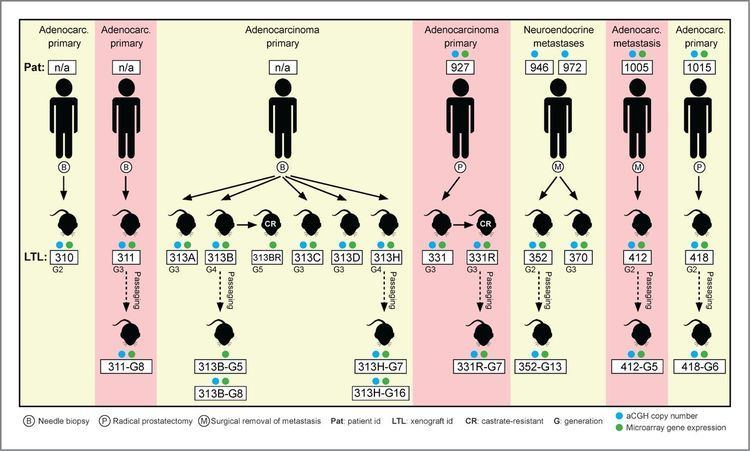
The first generation of mice receiving the patient's tumor fragments are commonly denoted F0. When the tumor-burden becomes too large for the F0 mouse, researchers passage the tumor over to the next generation of mice. Each generation thereafter is denoted F1, F2, F3…Fn. For drug development studies, expansion of mice after the F3 generation is often utilized after ensuring that the PDTX has not genetically or histologically diverged from the patient’s tumor.
Advantages over cancer cell lines
Cancer cell lines (CCL) are originally derived from patient tumors, but acquire the ability to proliferate within in vitro cell cultures. As a result of in vitro manipulation, CCL that have been traditionally used in cancer research undergo genetic transformations that are not restored when cells are allowed to grow in vivo. Because of the cell culturing process, which includes enzymatic environments and centrifugation, cells that are better adapted to survive in culture are selected, tumor resident cells and proteins that interact with cancer cells are eliminated, and the culture becomes phenotypically homogeneous.
When implanted into immunodeficient mice, CCL do not easily develop tumors and the result of any successfully grown tumor is a genetically divergent tumor unlike the heterogeneous patient tumor. Researchers are beginning to attribute the reason that only 5% of anti-cancer agents are approved by the Food and Drug Administration after pre-clinical testing to the lack of tumor heterogeneity and the absence of the human stromal microenvironment. Specifically, CCL-xenografts often are not predictive of the drug response in the primary tumors because CCL do not follow pathways of drug resistance or the effects of the microenvironment on drug response found in human primary tumors.
Many PDTX models have been successfully established for breast, prostate, colorectal, lung, and many other cancers because there are distinctive advantages when using PDTX over CCL for drug safety and efficacy studies as well as predicting patient tumor response to certain anti-cancer agents. Since PDTX can be passaged without in vitro processing steps, PDTX models allow the propagation and expansion of patient tumors without significant genetic transformation of tumor cells over multiple murine generations. Within PDTX models, patient tumor samples grow in physiologically-relevant tumor microenvironments that mimic the oxygen, nutrient, and hormone levels that are found in the patient’s primary tumor site. Furthermore, implanted tumor tissue maintains the genetic and epigenetic abnormalities found in the patient and the xenograft tissue can be excised from the patient to include the surrounding human stroma. As a result, numerous studies have found that PDTX models exhibit similar responses to anti-cancer agents as seen in the actual patient who provided the tumor sample. PDTX models are beneficial to use to study therapeutic responses to drugs because multiple therapies can be tested against one biopsy and pre- and post-treatment data can be acquired from the human biopsy and xenograft tissues, potentially sparing a patient from therapies that may not work.
Humanized-xenograft models
One prominent shortcoming of PDTX models is that immunodeficient mice must be used to prevent immune attacks against the xenotransplanted tumor. Therefore, a critical component of the known tumor microenvironment interaction is foregone. As a result, immunotherapies and anti-cancer agents that target the immune system components cannot be studied using PDTX models. Consequently, researchers are beginning to explore the use of humanized-xenograft models. Humanized-xenograft models are created by co-engrafting the patient tumor fragment and peripheral blood or bone marrow cells into a NOD/SCID mouse. The co-engraftment allows for reconstitution of the murine immune system enabling researchers to study the interactions between xenogenic human stroma and tumor environments in cancer progression and metastasis. However, these strategies have yet to be validated for most tumor types and there remains questions over whether the reconstituted immune system will behave in the same way as it does in the patient. For example, the immune system could be 'hyper-activated' due to exposure to mouse tissues in a similar fashion to graft versus host disease. Humanized-xenograft models for acute lymphoblastic leukemia and acute myeloid leukemia have been created.
Breast cancer
There have been many advances in breast cancer biology resulting in the classification of different molecular and genetic breast cancer subtypes including triple-negative and HER2-positive subtypes. Oncologists can use a patient’s breast cancer subtype to personalize cancer therapy schedules to better address the patient’s tumor distinct gene-expression profile. Utilizing PDTX triple negative breast cancer models, scientists found that aurora kinase inhibitors slows tumor growth rate and suppresses recurrence in a breast cancer subtype that has a high recurrence rate and poor survivability. Scientists have also found that breast cancer PDTX models are capable of predicting the prognosis of newly diagnosed women by observing the rate of tumor engraftment to determine if the patient tumor is aggressive.
Colorectal cancer
Colorectal PDTX models are relatively easy to establish and the models maintain genetic similarity of primary patient tumor for about 14 generations. In 2012, a study established 27 colorectal PDTX models that did not diverge from their respective human tumors in histology, gene expression, or KRAS/BRAF mutation status. Due to their stability, the 27 colorectal PDTX models may be able to serve as pre-clinical models in future drug studies. Drug resistance studies have been conducted using colorectal PDTX models. In one study, researchers found that the models predicted patient responsiveness to cetuximab with 90% accuracy. Another study identified the amplification of ERBB2 as another mechanism of resistance, and a putative new actionable target in treatments.
Pancreatic cancer
Researchers initially focused on using pancreatic PDTX models for drug studies to improve the process to develop predictive and pharmacodynamics end points for several molecularly targeted therapies. Other studies have been conducted to explore if pancreatic PDTX models can be used to guide the ongoing treatment of advance pancreatic cancer patient by screening multiple drugs to select the drug with most activity as the next line of treatment.
Pediatric cancer (neuroblastoma)
Researchers have established neuroblastoma PDXs by orthotopic implantation of patient tumor explants into immunodeficient mice. The PDXs retained the genotype and phenotype of patient tumors and exhibited substantial infiltrative growth and metastasis to distant organs including bone marrow. The researchers cultured PDX-derived neuroblastoma cells in vitro and the cells retained tumorigenic and metastatic capacity in vivo.
Challenges with PDTX model adaptation
There are several challenges that scientists face when developing or using PDTX models in research. For instance not all tumor samples will successfully engraft in the immunodeficient mouse. When engraftment does occur, clinical study protocols are difficult to standardize if engraftment rates vary. It is also expensive to house mice, maintain histopatholigcal cores for frequent testing, and to perform ex vivo passaging of tumors in mice with high tumor burdens.
With regard to using PDTX in personalized medicine, there are financial challenges. In the US, the cost to develop PDTX models is not covered by insurance and can potentially cost a patient $25,500 just for doctors to have access to the technology to potentially guide the patient's treatment.