
eMedicine article/371105 | ||
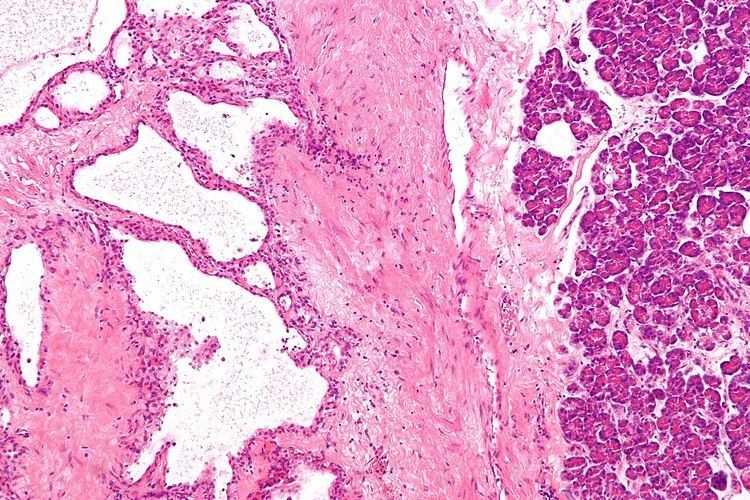 | ||
Pancreatic serous cystadenoma, also known as serous cystadenoma of the pancreas and serous microcystic adenoma, a benign tumour of pancreas. It is usually found in the head of the pancreas, and may be associated with von Hippel-Lindau syndrome.
Contents
In contrast to some of the other cyst-forming tumors of the pancreas (such as the intraductal papillary mucinous neoplasm and the mucinous cystic neoplasm), serous cystic neoplasms are almost always entirely benign. There are some exceptions; rare case reports have described isolated malignant serous cystadenocarcinomas. In addition, serous cystic neoplasms slowly grow, and if they grow large enough they can press on adjacent organs and cause symptoms.
Classification
Pathologists classify serous cystic neoplasms into two broad groups. Those that are benign, that have not spread to other organs, are designated "serous cystadenoma". Serous cystadenomas can be further sub-typed into microcystic, oligocystic (or macrocystic), solid, mixed serous-endocrine neoplasm, and VHL-associated serous cystic neoplasm. This latter classification scheme is useful because it highlights the range of appearances and the clinical associations of these neoplasms. Serous cystic neoplasms that have spread ("metastasized") to another organ are considered malignant and are designated "serous cystadenocarcinoma".
Diagnosis
Serous cystic neoplasms can come to clinical attention in a variety of ways. The most common symptoms are very non-specific and include abdominal pain, nausea and vomiting. In contrast to many of the other tumors of the pancreas, patients rarely develop jaundice (a yellowing of the skin and eyes caused by obstruction of the bile duct), or weight loss. These signs and symptoms are not specific for a serous cystic neoplasm, making it more difficult to establish a diagnosis. Doctors will therefore often order additional tests.
Once a doctor has reason to believe that a patient may have serous cystic neoplasm, he or she can confirm that suspicion using one of a number of imaging techniques. These include computerized tomography (CT), endoscopic ultrasound (EUS), and magnetic resonance cholangiopancreatography (MRCP). These tests will reveal a cystic mass within the pancreas. The cysts do not communicate with the larger pancreatic ducts. In some cases a fine needle aspiration (FNA) biopsy can be obtained to confirm the diagnosis. Fine needle aspiration biopsy can be performed through an endoscope at the time of endoscopic ultrasound, or it can be performed through the skin using a needle guided by ultrasound or CT scanning. A growing number of patients are now being diagnosed before they develop symptoms (asymptomatic patients). In these cases, the lesion in the pancreas is discovered accidentally (by chance) when the patient is being scanned (x-rayed) for another reason.
Treatment
These lesions rarely require surgery unless they are symptomatic or the diagnosis is in question. Since these lesions do not have malignant potential, long-term observation is unnecessary. Surgery can include the removal of the head of the pancreas (a pancreaticoduodenectomy), removal of the body and tail of the pancreas (a distal pancreatectomy), or rarely removal of the entire pancreas (a total pancreatectomy). In selected cases the surgery can be performed using minimally invasive techniques such as laparoscopy.