
 | ||
Outpatient commitment (more commonly known as Assisted Outpatient Treatment (AOT)) refers to state mental health laws that create civil court procedure wherein a judge orders a person with severe mental illness to adhere to an outpatient treatment plan designed to prevent relapse and dangerous deterioration. Assisted Outpatient Commitment allows the assisted involuntary treatment of individuals diagnosed with severe mental disorders who are living in the community and experiencing a mental illness crisis that requires intervention to prevent further deterioration that is harmful to themselves or others, rather than detained in hospital or incarcerated. The individual may be subject to rapid recall to hospital, including medication over objection, if the conditions of the plan/order are broken, and the person's mental health deteriorates. This generally means taking psychiatric medication as directed and may also include attending appointments with a mental health professional, and sometimes even not to take non-prescribed illicit drugs and not associate with certain people or in certain places deemed to have been linked to a deterioration in mental health in that individual.
Contents
- History
- Evidence
- Danger and violence reduced
- Consumer outcomes improved
- Improved access to services
- Racial neutrality
- Court orders add value
- AOT improves the likelihood that providers will serve seriously mentally ill
- AOT improves service engagement
- Individuals in AOT stay in treatment after AOT ends
- Controversy
- Proponents
- Opponents
- References
In the United States the term "assisted outpatient treatment" or "AOT" is often used and refers to a process whereby a judge orders a qualifying person with symptoms of severe untreated mental illness to adhere to a mental health treatment plan while living in the community. The plan typically includes medication and may include other forms of treatment as well. In England the Mental Health Act 2007 introduced "community treatment orders (CTOs)".
In Australia they are also called community treatment orders and last for a maximum of twelve months but can be renewed after review by a tribunal. Criteria for outpatient commitment are established by law, which vary among nations and, in the U.S., from state to state. Some require court hearings and others require that treating psychiatrists comply with a set of requirements before compulsory treatment is instituted.
When a court process is not required, there is usually a form of appeal to the courts or appeal to or scrutiny by tribunals set up for that purpose. Community treatment laws have generally followed the worldwide trend of community treatment. See mental health law for details of countries which do not have laws that regulate compulsory treatment.
History
Discussions of "outpatient commitment" began in the psychiatry community in the 1980s following deinstitutionalization, a trend that led to the widespread closure of public psychiatric hospitals and resulted in the discharge of large numbers of people with mental illness to the community. In the last decade of the 20th century and the first of the 21st, "outpatient commitment" laws were passed in a number of U.S. states and jurisdictions in Canada.
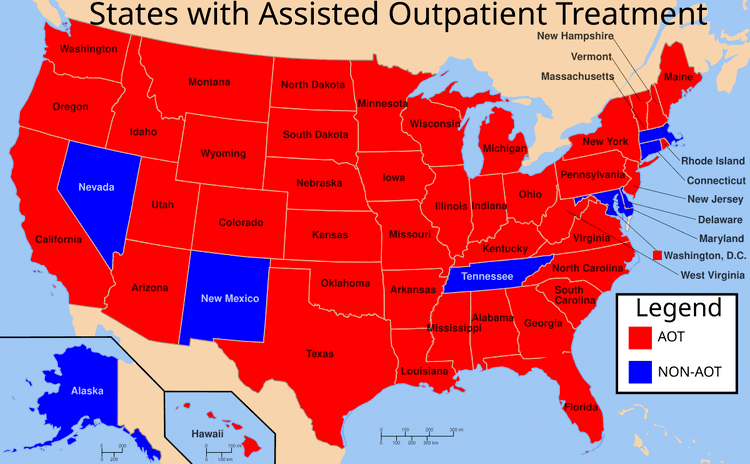
By the end of 2010, 44 U.S. states had enacted some version of an outpatient commitment law. In some cases, passage of the laws followed widely publicized tragedies, such as the murders of Laura Wilcox and Kendra Webdale.
Research published in 2013 showed that Kendra's Law in New York, which served about 2,500 patients at a cost of $32 million, had positive results in terms of net cost, reduced hospitalization, reduced arrests, use of outpatient treatment and use of medication. About $125 million is also spent annually on improved outpatient treatment for patients who are not subject to the law. In contrast to New York, despite wide adoption of outpatient commitment, the programs were generally not adequately funded.
Evidence
A 2011 meta-analytical review consisted of two RCTs, one a 1999 study done in New York and the other a 2001 study done in North Carolina, found that outpatient commitment "results in no significant difference in service use, social functioning or quality of life compared with standard care." The authors of this meta-analysis note in their 2012 update on Cochrane Reviews that five recently published studies are currently awaiting classification and may alter their findings.
“Although numerous AOT programs currently operate across the United States, it is clear that the intervention is vastly underutilized."
AOT “programs improve adherence with outpatient treatment and have been shown to lead to significantly fewer emergency commitments, hospital admissions, and hospital days as well as a reduction in arrests and violent behavior.”
Assisted outpatient treatment is an effective crime prevention program.
“For those who received AOT, the odds of any arrest were 2.66 times greater (p<.01) and the odds of arrest for a violent offense 8.61 times greater (p<.05) before AOT than they were in the period during and shortly after AOT. The group never receiving AOT had nearly double the odds (1.91, p<.05) of arrest compared with the AOT group in the period during and shortly after assignment.”
“The odds of arrest for participants currently receiving AOT were nearly two-thirds lower (OR=.39, p<.01) than for individuals who had not yet initiated AOT or signed a voluntary service agreement.”
“The likelihood of psychiatric hospital admission was significantly reduced by approximately 25% during the initial six-month court order…and by over one-third during a subsequent six-month renewal of the order…. Similar significant reductions in days of hospitalization were evident during initial court orders and subsequent renewals…. Improvements were also evident in receipt of psychotropic medications and intensive case management services. Analysis of data from case manager reports showed similar reductions in hospital admissions and improved engagement in services.”
Kendra’s Law has lowered risk of violent behaviors, reduced thoughts about suicide, and enhanced capacity to function despite problems with mental illness. Patients given mandatory outpatient treatment—who were more violent to begin with—were nevertheless four times less likely than members of the control group to perpetrate serious violence after undergoing treatment. Patients who underwent mandatory treatment reported higher social functioning and slightly less stigma, rebutting claims that mandatory outpatient care is a threat to self-esteem.
Danger and violence reduced
55% fewer recipients engaged in suicide attempts or physical harm to self. 47% fewer physically harmed others. 46% fewer damaged or destroyed property. 43% fewer threatened physical harm to others. Overall, the average decrease in harmful behaviors was 44%.
Consumer outcomes improved
74% fewer participants experienced homelessness. 77% fewer experienced psychiatric hospitalization. 56% reduction in length of hospitalization. 83% fewer experienced arrest. 87% fewer experienced incarceration. 49% fewer abused alcohol. 48% fewer abused drugs. Consumer participation and medication compliance improved The number of individuals exhibiting good adherence to meds increased 51%. The number of individuals exhibiting good service engagement increased 103%. Consumer perceptions were positive 75% reported that AOT helped them gain control over their lives. 81% said AOT helped them get and stay well. 90% said AOT made them more likely to keep appointments and take meds. 87% of participants said they were confident in their case manager’s ability. 88% said they and their case manager agreed on what was important to work on
Improved access to services
AOT has been instrumental in increasing accountability at all system levels regarding delivery of services to high need individuals. Community awareness of AOT has resulted in increased outreach to individuals who had previously presented engagement challenges to mental health service providers.” “Improved treatment plan development, discharge planning, and coordination of service planning. Processes and structures developed for AOT have resulted in improvements to treatment plans that more appropriately match the needs of individuals who have had difficulties using mental health services in the past.” “Improved collaboration between mental health and court systems. As AOT processes have matured, professionals from the two systems have improved their working relationships, resulting in greater efficiencies, and ultimately, the conservation of judicial, clinical, and administrative resources. There is now an organized process to prioritize and monitor individuals with the greatest need; AOT ensures greater access to services for individuals whom providers have previously been reluctant to serve; There is now increased collaboration between inpatient and community-based providers.”
In New York City net costs declined 50% in the first year after assisted outpatient treatment began and an additional 13% in the second year. In non-NYC counties, costs declined 62% in the first year and an additional 27% in the second year. This was in spite of the fact that psychotropic drug costs increased during the first year after initiation of assisted outpatient treatment, by 40% and 44% in the city and five-county samples, respectively. The increased community-based mental health costs were more than offset by the reduction in inpatient and incarceration costs. Cost declines associated with assisted outpatient treatment were about twice as large as those seen for voluntary services.
“In all three regions, for all three groups, the predicted probability of an M(edication) P(ossession) R(atio) ≥80% improved over time (AOT improved by 31–40 percentage points, followed by enhanced services, which improved by 15–22 points, and ‘neither treatment,’ improving 8–19 points). Some regional differences in MPR trajectories were observed.”
“In tandem with New York’s AOT program, enhanced services increased among involuntary recipients, whereas no corresponding increase was initially seen for voluntary recipients. In the long run, however, overall service capacity was increased, and the focus on enhanced services for AOT participants appears to have led to greater access to enhanced services for both voluntary and involuntary recipients.”
“We find that New York State’s AOT Program improves a range of important outcomes for its recipients, apparently without feared negative consequences to recipients.”
Racial neutrality
“We find no evidence that the AOT Program is disproportionately selecting African Americans for court orders, nor is there evidence of a disproportionate effect on other minority populations. Our interviews with key stakeholders across the state corroborate these findings.”
Court orders add value
“The increased services available under AOT clearly improve recipient outcomes, however, the AOT court order, itself, and its monitoring do appear to offer additional benefits in improving outcomes.”
AOT improves the likelihood that providers will serve seriously mentally ill
“It is also important to recognize that the AOT order exerts a critical effect on service providers stimulating their efforts to prioritize care for AOT recipients.”
AOT improves service engagement
“After 12 months or more on AOT, service engagement increased such that AOT recipients were judged to be more engaged than voluntary patients. This suggests that after 12 months or more, when combined with intensive services, AOT increases service engagement compared to voluntary treatment alone.” Consumers Approve. Despite being under a court order to participate in treatment, current AOT recipients feel neither more positive nor more negative about their treatment experiences than comparable individuals who are not under AOT.”
Individuals in AOT stay in treatment after AOT ends
“When the court order was for seven months or more, improved medication possession rates and reduced hospitalization outcomes were sustained even when the former AOT recipients were no longer receiving intensive case coordination services.”
In Nevada County, CA, AOT (“Laura’s Law”) decreased the number of Psychiatric Hospital Days 46.7%, the number of Incarceration Days 65.1%, the number of Homeless Days 61.9%, and the number of Emergency Interventions 44.1%. Laura’s Law implementation saved $1.81–$.2.52 for every dollar spent, and receiving services under Laura’s Law caused a “reduction in actual hospital costs of $213,300” and a “reduction in actual incarceration costs of $75,600.”
In Los Angeles, CA, the AOT pilot program reduced incarceration 78%, hospitalization 86%, hospitalization after discharge from the program 77%, and cut taxpayer costs 40%.
In North Carolina, AOT reduced the percentage of persons refusing medications to 30%, compared to 66% of patients not under AOT.
In Ohio, AOT increased attendance at outpatient psychiatric appointments from 5.7 to 13.0 per year. It increased attendance at day treatment sessions from 23 to 60 per year. “During the first 12 months of outpatient commitment, patients experienced significant reductions in visits to the psychiatric emergency service, hospital admissions, and lengths of stay compared with the 12 months before commitment.”
In Arizona, “71% [of AOT patients] . . . voluntarily maintained treatment contacts six months after their orders expired” compared with “almost no patients” who were not court-ordered to outpatient treatment.
In Iowa, “it appears as though outpatient commitment promotes treatment compliance in about 80% of patients… After commitment is terminated, about ¾ of that group remain in treatment on a voluntary basis.”
In New Jersey, Kim Veith, director of clinical services at Ocean Mental Health Services, noted the AOT pilot program performed “beyond wildest dreams.” AOT reduced hospitalizations, shortened inpatient stays, reduced crime and incarceration, stabilized housing, and reduced homelessness. Of clients who were homeless, 20% are now in supportive housing, 40% are in boarding homes, and 20% are living successfully with family members.
“Subjects who were ordered to outpatient commitment were less likely to be criminally victimized than those who were released without outpatient commitment.”
“We found no evidence of racial bias. Defining the target population as public-system clients with multiple hospitalizations, the rate of application to white and black clients approaches parity.”
The British Journal of Psychiatry stated in 2013 "The current evidence from RCTs suggests that CTOs(Community treatment orders) do not reduce readmission rates over 12 months."
Controversy
Proponents have argued that outpatient commitment improves mental health, increases the effectiveness of treatment, lowers incidence of homelessness, arrest, incarceration and hospitalization and reduces costs. Opponents of outpatient commitment laws argue that they unnecessarily limit freedom, force people to ingest dangerous medications, or are applied with racial and socioeconomic biases.
Proponents
While many outpatient commitment laws have been passed in response to violent acts committed by people with mental illness, most proponents involved in the outpatient commitment debate base their arguments on the quality of life and cost associated with untreated mental illness and "revolving door patients" who experience a cycle of hospitalization, treatment and stabilization, release, and decompensation. While the cost of repeated hospitalzations is indisputable, quality-of-life arguments rest on an understanding of mental illness as an undesirable and dangerous state of being. Outpatient commitment proponents point to studies performed in North Carolina and New York that have found some positive impact of court-ordered outpatient treatment. Proponents include: Substance Abuse and Mental Health Services Administration (SAMHSA), U.S. Department of Justice, Agency for Healthcare Research and Quality (AHRQ), U. S Department of Health and Human Services, American Psychiatric Association, National Alliance on Mental Illness, International Association of Chiefs of Police. SAMHSA included Assisted Outpatient Treatment in their National Registry of Evidence Based Program and Practices. Crime Solutions: Management Strategies to Reduce Psychiatric Readmissions
Opponents
Outpatient commitment opponents make several varied arguments. Some dispute the positive effects of compulsory treatment, questioning the methodology of studies that show effectiveness. Others highlight negative effects of treatment. Still others point to disparities in the way these laws are applied.
The opponents claim they are giving medication to the patient, but there are no brain chemical imbalances to correct in "mental illness". Our ability to control ourselves and reason comes from the mind, and the brain is being reduced in size from the psychiatric medications.
The slippery slope argument of "If government bodies are given power, they will use it in excess." was proven when 350-450 CTO's were expected to be issued in 2008 and more than five times that number were issued in the first few months. Every year there are increasing numbers of people subject to CTO's.
The psychiatric survivors movement opposes compulsory treatment on the basis that the ordered drugs often have serious or unpleasant side-effects such as tardive dyskinesia, neuroleptic malignant syndrome, excessive weight gain leading to diabetes, addiction, sexual side effects, and increased risk of suicide. The New York Civil Liberties Union has denounced what they see as racial and socioeconomic biases in the issuing of outpatient commitment orders. The main opponents to any kind of coercion, including the outpatient commitment and any other form of involuntary commitment, are Giorgio Antonucci and Thomas Szasz.