
Specialty endocrinology OMIM 304150 | ICD-10 E83.0 DiseasesDB 33413 | |
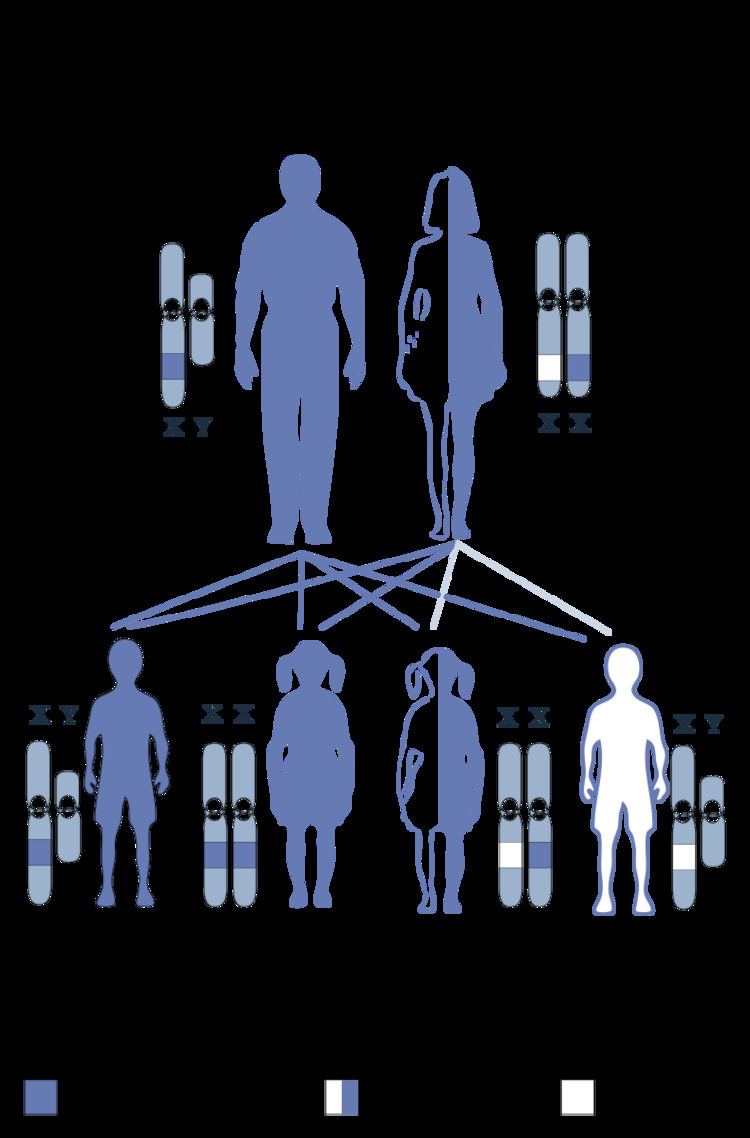 | ||
Occipital horn syndrome (OHS), formerly considered a variant of Ehlers-Danlos syndrome, is an X-linked recessive connective tissue disorder. It is caused by a deficiency in the transport of the essential mineral copper, associated with mutations in the ATP7A gene. Only about 2/3 of children with OHS are thought to have genetically inherited the disorder; the other 1/3 do not have the disease in their family history. Since the disorder is X-linked recessive the disease affects more males. This is because they do not have a second X chromosome, unlike females, so essentially are lacking the 'backup' copy with proper function. Females are much more likely to be carriers only. For a female to be affected they must carry two defective X chromosomes, not just one. The disorder is considered a milder variant of Menkes disease.
Contents
Signs/symptoms
It is characterized by a deficiency in biliary copper excretion that causes deformations in the skeleton. These include projections on the back of the skull (parasagittal bone exostoses arising from the occipital bone—the so-called "occipital horns") as well as deformities of the elbow, radial head dislocation, hammer-shaped lateral ends of the clavicles, and abnormalities of the hips and pelvis. OHS presents in early to middle childhood. Children may present with features such as:
Causes
OHS is a milder allelic variant of Menkes disease, having a later age of onset and being associated with far less severe central neurodegeneration. The milder nature of OHS is often attributable to ‘leaky’ splice junction mutations that allow 20–30% of ATP7A messenger RNA (mRNA) transcripts to be correctly processed. As in cases of Menkes disease, individuals with OHS manifest connective tissue abnormalities resulting from deficient activity of lysyl oxidase, a copper-requiring enzyme that normally deaminates lysine and hydroxylysine in the first step of collagen crosslink formation. Such individuals also often endure inconvenient dysautonomic signs and symptoms related to a partial deficiency in dopamine-β-hydroxylase (DBH) activity. DBH, another copper-dependent enzyme, normally converts dopamine to norepinephrine, a crucial neurotransmitter in norepinephrinergic neurons. A natural mouse model of OHS, the so-called mottled blotchy model, recapitulates the connective tissue abnormalities, DBH deficiency and mild CNS damage seen in humans.
Treatment
Courses of treatment for children with is dependent upon the severity of their case. Children with OHS often receive physical and occupational therapy. They may require a feeding tube to supplement nourishment if they are not growing enough. In an attempt to improve the neurological condition (seizures) copper histidine or copper chloride injections can be given early in the child’s life. However, copper histidine injections have been shown ineffective in studies of copper metabolic-connective tissue disorders such as OHS.