
ICD-9-CM 35.8 | ||
 | ||
The Norwood procedure is a three-stage heart surgery to create a new functional systemic circuit in patients with hypoplastic left heart syndrome. Stage 1 of the Norwood procedure involves atrial septectomy and transection and ligation of the distal main pulmonary artery. The proximal pulmonary artery is then connected to the hypoplastic aortic arch, while the coarcted segment of the aorta is repaired. An aortopulmonary shunt is created to connect the aorta to the main pulmonary artery to provide pulmonary blood flow. Stage 2 of the Norwood procedure is separation of the systemic and pulmonary circulation once pulmonary vascular resistance has fallen, by removing the aortopulmonary shunt followed by creation of a bidirectional SVC-pulmonary shunt, also known as a Glenn procedure. Stage 3 of the Norwood procedure is creation of a modified Fontan procedure. The first successful use of the procedure was reported by Dr. William Imon Norwood, Jr. (1941 – ) and colleagues in 1981.
Contents
Cardiopulmonary bypass is required.
Indications
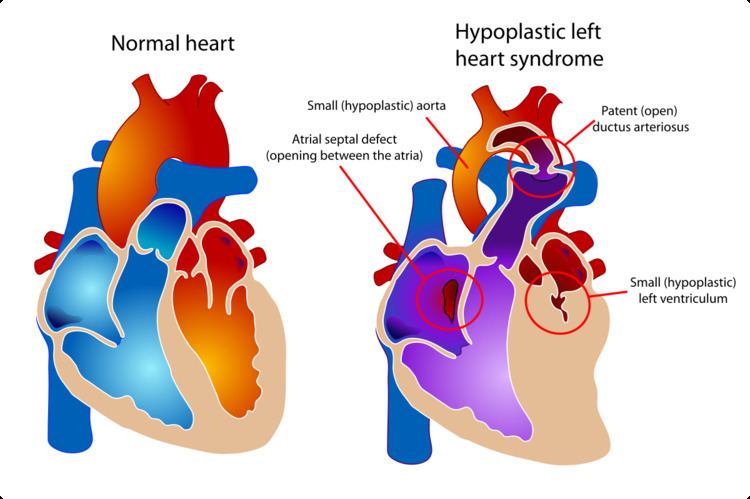
This procedure is most often performed to treat hypoplastic left heart syndrome, certain types of mitral atresia, or other conditions that result in single ventricle circulation.
In these conditions, the most urgent problem is that the heart is unable to pump blood to the systemic circulation (i.e. to the body). The goal of the Norwood procedure is to connect the single ventricle to the systemic circulation. To accomplish this, blood flow to the lungs is disrupted, and therefore an alternative path must be created to supply the lungs.
Process
Entry to the body cavity for the Norwood procedure is gained by a vertical incision above the sternum. Separation of the sternum is necessary.
This surgery is complex and may vary slightly depending on the diagnosis and overall condition of the heart.
The surgery on the heart can be divided into two main steps.
Providing systemic circulation
The main pulmonary artery is separated from the left and right portions of the pulmonary artery and joined with the upper portion of the aorta. Widening of the pulmonary artery is often necessary, and may be accomplished by using the patient's existing biological tissue, or appropriate animal tissue. This allows the blood, a mixture of oxygenated and deoxygenated, to be pumped to the body via the morphologic right ventricle, through the pulmonary valve.
Providing pulmonary circulation
Since the remainder of the pulmonary artery is now disconnected from the heart, one of a few techniques must be used to supply blood to the lungs:
After this first step (switching the right ventricle in functional position of the absent left ventricle) children generally proceed down the path to a Fontan procedure.