
Specialty Ophthalmology ICD-9-CM 367.1 MedlinePlus 001023 | ICD-10 H52.1 DiseasesDB 8729 | |
 | ||
Synonyms myopia, short-sightedness, near-sighted | ||
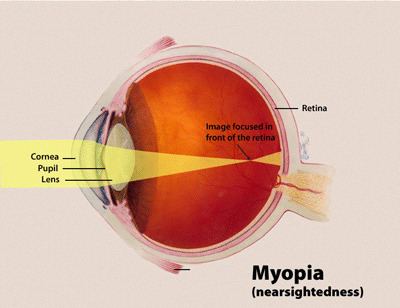
Near-sightedness, also known as short-sightedness and myopia, is a condition of the eye where light focuses in front of, instead of on, the retina. This causes distant objects to be blurry while close objects appear normal. Other symptoms may include headaches and eye strain. Severe near-sightedness increases the risk of retinal detachment, cataracts, and glaucoma.
Contents
- Signs and symptoms
- Causes
- Near work hypothesis
- Visual stimuli hypothesis
- Other risk factors
- Diagnosis
- By cause
- Clinical entity
- Degree
- Age at onset
- Prevention
- Glasses and contact lenses
- Medication
- Other methods
- Management
- Eyeglasses
- Refractive surgery
- PRK LASEK
- LASIK
- Phakic intra ocular lens
- Alternative medicine
- Epidemiology
- Asia
- Europe
- North America
- Oceania Australia
- South America
- Society and culture
- Correlations
- Research
- Genetic basis for myopia
- Visual environment
- Etymology
- References
The underlying cause is believed to be a combination of genetic and environmental factors. Risk factors include doing work that involves focusing on close objects, greater time spent indoors, and a family history of the condition. It is also associated with a high socioeconomic class. The underlying mechanism involves the length of the eyeball being too long or less commonly the lens being too strong. It is a type of refractive error. Diagnosis is by eye examination.
There is tentative evidence that near-sightedness can be prevented by having young children spend more time outside. This may be related to natural light exposure. Near-sightedness can be corrected with eyeglasses, contact lenses, or surgery. Eyeglasses are the easiest and safest method of correction. Contact lenses can provide a wider field of vision; however are associated with a risk of infection. Refractive surgery permanently changes the shape of the cornea.
Near-sightedness is the most common eye problem and is estimated to affect 1.5 billion people (22% of the population). Rates vary significantly in different areas of the world. Rates among adults are between 15 and 49%. Rates are similar in males and females. Among children it affects 1.2% of rural Nepalese, 4% of South Africans, 12% of Americans, and 37% in some large Chinese cities. Rates have increased since the 1950s. Uncorrected near-sightedness is one of the most common causes of vision loss globally along with cataracts, macular degeneration, and vitamin A deficiency.
Signs and symptoms
Myopia presents with blurry distance vision, but generally gives good near vision. In high myopia, even near vision is affected as objects must be extremely close to the eyes to see clearly, and people with myopia cannot read without their glasses prescribed for distance. On fundoscopic examination of the eye, the optic nerve appears to be tilted and an area of white sclera could be seen on next to the disc with a line of hyperpigmentation separating this area from normal retina. The macula will have some retinal pigmentary changes and sometimes will have subretinal hemorrhages. The retina in myopic patients is thin and thorough evaluation of the periphery might show retinal holes and lattice degeneration. In addition, people with myopia might develop choroidal neovascularization in the macula.
Causes
A 2012 review could not find strong evidence for any cause, although many theories have been discredited. Because twins and relatives are more likely to get myopia under similar circumstances, there must be a hereditary factor, but because myopia has been increasing so rapidly throughout the developed world, environmental factors must be more important.
“Near work” hypothesis
The "near work" hypothesis, also referred to as the “use-abuse theory” states that spending time involved in near work strains the eyes and increases the risk of myopia. Some studies support the hypothesis while other studies do not. While an association is present it is unclear if it is causal.
Quite similarly, it is still unclear what is the mechanism of emmetropization, that is, the mechanism by which the degree of hyperopia (far-sightedness) and myopia change during childhood, such that a farsighted eye tends to become less farsighted and a near-sighted eye tends to become less near-sighted in the course of development.
"Visual stimuli" hypothesis
Although not mutually exclusive with the other hypotheses presented, the visual stimuli hypothesis adds another layer of mismatch to explain the modern prevalence of myopia. There is evidence that lack of normal visual stimuli causes improper development of the eyeball. In this case, "normal" refers to the environmental stimuli that the eyeball evolved for over hundreds of millions of years. These stimuli would include diverse natural environments—the ocean, the jungle, the forest, and the savannah plains, among other dynamic visually exciting environments. Modern humans who spend most of their time indoors, in dimly or fluorescently lit buildings are not giving their eyes the appropriate stimuli to which they had evolved and may contribute to the development of myopia. Experiments where animals such as kittens and monkeys had their eyes sewn shut for long periods of time also show eyeball elongation, demonstrating that complete lack of stimuli also causes improper growth trajectories of the eyeball. Further research shows that people, and children especially, who spend more time doing physical exercise and outdoor activity have lower rates of myopia, relating the increased magnitude and complexity of the visual stimuli encountered during these types of activities.
There is preliminary evidence that the protective effect of outdoor activities on the development of myopia is due, at least in part, to the effect of daylight on the production and the release of retinal dopamine.
Other risk factors
In one study, heredity was an important factor associated with juvenile myopia, with smaller contributions from more near work, higher school achievement, and less time in sports activity.
Long hours of exposure to daylight appears to be a protective factor. Researchers at the University of Cambridge have found that a lack of outdoor play could be linked to myopia. Other personal characteristics, such as value systems, school achievements, time spent in reading for pleasure, language abilities, and time spent in sport activities all correlated to the occurrence of myopia in studies.
Diagnosis
A diagnosis of myopia is typically confirmed during an eye examination performed by a specialized doctor who is an expert in refractive conditions of the eye, the optometrist, or by an ophthalmologist or orthoptist. Frequently an autorefractor or retinoscope is used to give an initial objective assessment of the refractive status of each eye, then a phoropter is used to subjectively refine the patient's eyeglass prescription. Other types of refractive error are far-sightedness, astigmatism, and presbyopia.
By cause
Borish and Duke-Elder classified myopia by cause:
Elevation of blood-glucose levels can also cause edema (swelling) of the crystalline lens as a result of sorbitol (sugar alcohol) accumulating in the lens. This edema often causes temporary myopia (near-sightedness).
Clinical entity
Various forms of myopia have been described by their clinical appearance:
Degree
Myopia, which is measured in diopters by the strength or optical power of a corrective lens that focuses distant images on the retina, has also been classified by degree or severity:
Age at onset
Myopia is sometimes classified by the age at onset:
Prevention
The National Institutes of Health says there is no known way of preventing myopia, and the use of glasses or contact lenses does not affect its progression. There is no universally accepted method of preventing myopia; proposed procedures have not been studied for effectiveness.
Some suggest that more time spent outdoors during childhood is effective for prevention.
Various methods have been employed in an attempt to decrease the progression of myopia, although studies show mixed results. Many myopia treatment studies have a number of design drawbacks: small numbers, lack of adequate control group, and failure to mask examiners from knowledge of treatments used.
Glasses and contact lenses
The use of reading glasses when doing close work may provide success by reducing or eliminating the need to accommodate. Altering the use of eyeglasses between full-time, part-time, and not at all does not appear to alter myopia progression. The American Optometric Association's Clinical Practice Guidelines for Myopia refers to numerous studies which indicated the effectiveness of bifocal lenses and recommends it as the method for "Myopia Control". In some studies, bifocal and progressive lenses have not shown significant differences in altering the progression of myopia.
Medication
Anti-muscarinic topical medications in children under 18 years of age may slow the worsening of myopia. These treatments include pirenzepine gel, cyclopentolate eye drops, and atropine eye drops. While these treatments were shown to be effective in slowing the progression of myopia, side effects included light sensitivity and near blur.
Other methods
Scleral reinforcement surgery is aimed to cover the thinning posterior pole with a supportive material to withstand intraocular pressure and prevent further progression of the posterior staphyloma. The strain is reduced, although damage from the pathological process cannot be reversed. By stopping the progression of the disease, vision may be maintained or improved.
Management
Optical correction using glasses or contact lenses is the most common approach; other approaches include drugs (mostly atropine), vision therapy, orthokeratology, and refractive surgery.
Eyeglasses
The corrective lenses decrease the power of the eye's optics (i.e. they have negative power by being concave lenses; they are the opposite of a magnifying glass). The power of any lens system is expressed in diopters, as the reciprocal of its focal length in meters. Corrective lenses for near-sightedness have negative powers; the more negative the value then the more severe is the near-sightedness.
For people with a high degree of myopia, very strong eyeglass prescriptions are needed to correct the focus error. However, strong eyeglass prescriptions have a negative side effect in that off-axis viewing of objects, away from the center of the lens, results in prismatic movement and separation of colors, known as chromatic aberration. This prismatic distortion is visible to the wearer as color fringes around strongly contrasting colors. The fringes move around as the wearer's gaze through the lenses changes, and the prismatic shifting reverses on either side, above, and below the exact center of the lenses. Color fringing can make accurate drawing and painting difficult for users of strong eyeglass prescriptions.
Strongly near-sighted wearers of contact lenses do not experience chromatic aberration because the lens moves with the cornea, as the eye turns, and always stays centered in the middle of the wearer's gaze.
Refractive surgery
Refractive surgery includes procedures which alter the corneal curvature or which add additional refractive means inside the eye.
PRK / LASEK
Photorefractive keratectomy (PRK) involves ablation of corneal tissue from the corneal surface using an excimer laser. The amount of tissue ablation corresponds to the amount of myopia. While PRK is a relatively safe procedure for up to 6 dioptres of myopia, the recovery phase post-surgery is usually painful.
LASIK
In a LASIK pre-procedure, a corneal flap is cut into the cornea and lifted to allow the excimer laser beam access to the exposed corneal tissue. After that, the excimer laser ablates the tissue according to the required correction. When the flap again covers the cornea, the change in curvature generated by the laser ablation proceeds to the corneal surface. Though LASIK is usually painless and involves a short rehabilitation period post-surgery, it can potentially result in flap complications and loss of corneal stability (post-LASIK keratectasia).
Phakic intra-ocular lens
Instead of modifying the corneal surface, as in laser vision correction (LVC), this procedure involves implanting an additional lens inside the eye (i.e., in addition to the already existing natural lens). While it usually results in good control of the refractive change, it can induce potential serious long-term complications such as glaucoma, cataract and endothelial decompensation.
Alternative medicine
A number of alternative therapies have been claimed to improve myopia, including vision therapy, "behavioural optometry", various eye exercises and relaxation techniques, and the Bates method. Scientific reviews have concluded that there was "no clear scientific evidence" that eye exercises are effective in treating near-sightedness and as such they "cannot be advocated."
In the 1980s and 1990s, biofeedback created interest as a possible treatment for near-sightedness. A 1997 review of this biofeedback research concluded "controlled studies to validate such methods ... have been rare and contradictory." One study found that myopes could improve their visual acuity with biofeedback training, but that this improvement was "instrument-specific" and did not generalize to other measures or situations. In another study, an "improvement" in visual acuity was found, but the authors concluded this could be a result of subjects learning the task. Finally, in an evaluation of a training system designed to improve acuity, "no significant difference was found between the control and experimental subjects".
Epidemiology
Global refractive errors have been estimated to affect 800 million to 2.3 billion. The incidence of myopia within sampled population often varies with age, country, sex, race, ethnicity, occupation, environment, and other factors. Variability in testing and data collection methods makes comparisons of prevalence and progression difficult.
The prevalence of myopia has been reported as high as 70–90% in some Asian countries, 30–40% in Europe and the United States, and 10–20% in Africa. Myopia is about twice as common in Jews than in people of non-Jewish ethnicity. Myopia is less common in African people and associated diaspora. In Americans between the ages of 12 and 54, myopia has been found to affect African Americans less than Caucasians.
Asia
In some parts of Asia, myopia is very common.
Europe
North America
Myopia is common in the United States, with research suggesting this condition has increased dramatically in recent decades. In 1971–1972, the National Health and Nutrition Examination Survey provided the earliest nationally representative estimates for myopia prevalence in the U.S., and found the prevalence in persons aged 12–54 was 25.0%. Using the same method, in 1999–2004, myopia prevalence was estimated to have climbed to 41.6%.
A study of 2,523 children in grades 1 to 8 (age, 5–17 years) found nearly one in 10 (9.2%) have at least − 0.75 diopters of myopia. In this study, 12.8% had at least +1.25 D hyperopia (farsightedness), and 28.4% had at least 1.00-D difference between the two principal meridians (cycloplegic autorefraction) of astigmatism. For myopia, Asians had the highest prevalence (18.5%), followed by Hispanics (13.2%). Caucasian children had the lowest prevalence of myopia (4.4%), which was not significantly different from African Americans (6.6%).
A recent review found 25.4% of Americans aged 40 or over have at least −1.00 diopters of myopia and 4.5% have at least −5.00 diopters.
Oceania (Australia)
In Australia, the overall prevalence of myopia (worse than −0.50 diopters) has been estimated to be 17%. In one recent study, less than one in 10 (8.4%) Australian children between the ages of four and 12 were found to have myopia greater than −0.50 diopters. A recent review found 16.4% of Australians aged 40 or over have at least −1.00 diopters of myopia and 2.8% have at least −5.00 diopters.
South America
In Brazil, a 2005 study estimated 6.4% of Brazilians between the ages of 12 and 59 had −1.00 diopter of myopia or more, compared with 2.7% of the indigenous people in northwestern Brazil. Another found nearly 1 in 8 (13.3%) of the students in the city of Natal were myopic.
Society and culture
The terms "myopia" and "myopic" (or the common terms "short-sightedness" or "short-sighted", respectively) have been used metaphorically to refer to cognitive thinking and decision making that is narrow in scope or lacking in foresight or in concern for wider interests or for longer-term consequences. It is often used to describe a decision that may be beneficial in the present, but detrimental in the future, or a viewpoint that fails to consider anything outside a very narrow and limited range. Hyperopia, the biological opposite of myopia, may also be used metaphorically for a value system or motivation that exhibits "farsighted" or possibly visionary thinking and behavior; that is, emphasizing long-term interests at the apparent expense of near-term benefit.
Correlations
Numerous studies have found correlations between myopia, on the one hand, and intelligence and academic achievement, on the other; it is not clear whether there is a causal relationship.
Research
Normally eye development is largely genetically controlled, but it has been shown that the visual environment is an important factor in determining ocular development. Some research suggests that some cases of myopia may be inherited from one's parents.
Genetic basis for myopia
Genetically, linkage studies have identified 18 possible loci on 15 different chromosomes that are associated with myopia, but none of these loci are part of the candidate genes that cause myopia. Instead of a simple one-gene locus controlling the onset of myopia, a complex interaction of many mutated proteins acting in concert may be the cause. Instead of myopia being caused by a defect in a structural protein, defects in the control of these structural proteins might be the actual cause of myopia. A collaboration of all myopia studies worldwide, identified 16 new loci for refractive error in individuals of European ancestry, of which 8 were shared with Asians. The new loci include candidate genes with functions in neurotransmission, ion transport, retinoic acid metabolism, extracellular matrix remodeling and eye development. The carriers of the high-risk genes have a tenfold increased risk of myopia.
Human population studies suggest that contribution of genetic factors accounts for 60%-90% of variance in refraction. However, the currently-identified variants account for only a small fraction of myopia cases suggesting the existence of a large number of yet unidentified low-frequency or small-effect variants, which underlie the majority of myopia cases.
Visual environment
To induce myopia in lower as well as higher vertebrates, translucent goggles can be sutured over the eye, either before or after natural eye opening. Form-deprived myopia (FDM) induced with a diffuser, like the goggles mentioned, shows significant myopic shifts. Imposing retinal blur (or defocus) with positive (myopic defocus, that causes the image to be focussed in front of the retina) and negative lenses (hyperopic defocus, that causes the image to be focussed behind the retina) has also been shown to result in predictable changes in eye growth of various animal models, whereby the eye alters its growth to effectively eliminate the lens induced blur. Anatomically, the changes in axial length of the eye seem to be the major factor contributing to this type of myopia. Diurnal growth rhythms of the eye have also been shown to play a large part in FDM, and have been implicated in refractive error development of human eyes. Chemically, daytime retinal dopamine levels drop about 30%.
Normal eyes grow during the day and shrink during the night, but occluded eyes are shown to grow both during the day and the night. Because of this, FDM is a result of the lack of growth inhibition at night rather than the expected excessive growth during the day, when the actual light deprivation occurred. Elevated levels of retinal dopamine transporter (which is directly involved in controlling retinal dopamine levels) in the RPE have been shown to be associated with FDM.
Etymology
The term myopia is of Koine Greek origin: μυωπία myōpia (or μυωπίασις myōpiasis) "short-sight(-ness)", from Ancient Greek μύωψ myōps "short-sighted (man), (man) with eyes getting shut", from μύειν myein "to shut the eyes" and ὤψ ōps "eye, look, sight" (GEN ὠπός ōpos). The opposite of myopia in English is hyperopia (long-sightedness).