
 | ||
The medical history or (medical) case history (also called epicrisis – typically discharge summary to referring GP, or anamnesis, especially historically) (often abbreviated hx or Hx) of a patient is information gained by a physician by asking specific questions, either of the patient or of other people who know the person and can give suitable information (in this case, it is sometimes called heteroanamnesis), with the aim of obtaining information useful in formulating a diagnosis and providing medical care to the patient. The medically relevant complaints reported by the patient or others familiar with the patient are referred to as symptoms, in contrast with clinical signs, which are ascertained by direct examination on the part of medical personnel. Most health encounters will result in some form of history being taken. Medical histories vary in their depth and focus. For example, an ambulance paramedic would typically limit their history to important details, such as name, history of presenting complaint, allergies, etc. In contrast, a psychiatric history is frequently lengthy and in depth, as many details about the patient's life are relevant to formulating a management plan for a psychiatric illness.
Contents
The information obtained in this way, together with the physical examination, enables the physician and other health professionals to form a diagnosis and treatment plan. If a diagnosis cannot be made, a provisional diagnosis may be formulated, and other possibilities (the differential diagnoses) may be added, listed in order of likelihood by convention. The treatment plan may then include further investigations to clarify the diagnosis.
Process
A practitioner typically asks questions to obtain the following information about the patient:
History-taking may be comprehensive history taking (a fixed and extensive set of questions are asked, as practiced only by health care students such as medical students, physician assistant students, or nurse practitioner students) or iterative hypothesis testing (questions are limited and adapted to rule in or out likely diagnoses based on information already obtained, as practiced by busy clinicians). Computerized history-taking could be an integral part of clinical decision support systems.
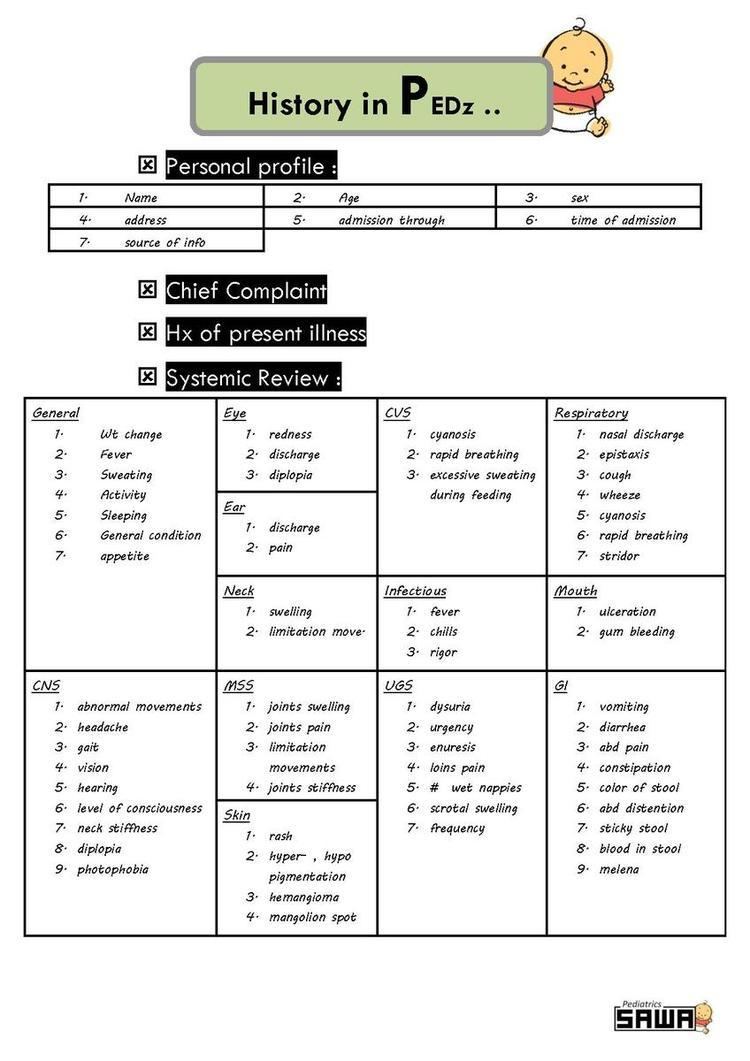
Review of systems
Whatever system a specific condition may seem restricted to, all the other systems are usually reviewed in a comprehensive history. The review of systems often includes all the main systems in the body that may provide an opportunity to mention symptoms or concerns that the individual may have failed to mention in the history. Health care professionals may structure the review of systems as follows:
Inhibiting factors
Factors that inhibit a proper medical history taking include physical inability of the patient to communicate with the physician, such as unconsciousness and communication disorders. In such cases, it may be necessary to perform a so-called heteroanamnesis of other people who know the person and can give suitable information, which, however, generally is more limited than a direct anamnesis.
Medical history taking may also be impaired by various factors impeding a proper doctor-patient relationship, such as transitions to physicians that are unfamiliar to the patient.
History taking of issues related to sexual or reproductive medicine may be inhibited by a reluctance of the patient to disclose intimate or uncomfortable information. Even if such an issue is on the patient's mind, he or she often doesn't start talking about such an issue without the physician initiating the subject by a specific question about sexual or reproductive health. Some familiarity with the doctor generally makes it easier for patients to talk about intimate issues such as sexual subjects, but for some patients, a very high degree of familiarity may make the patient reluctant to reveal such intimate issues. When visiting a health provider about sexual issues, having both partners of a couple present is often necessary, and is typically a good thing, but may also prevent the disclosure of certain subjects, and, according to one report, increases the stress level.
Computer-assisted history taking
Computer-assisted history taking systems have been available since the 1960s. However, their use remains variable across healthcare delivery systems.
One advantage of using computerized systems as an auxiliary or even primary source of medically related information is that patients may be less susceptible to social desirability bias. For example, patients may be more likely to report that they have engaged in unhealthy lifestyle behaviors. Another advantage of using computerized systems is that they allow easy and high-fidelity portability to a patient's electronic medical record. Also an advantage is that it saves money and paper.
One disadvantage of current (2012) medical history systems is that they cannot detect non-verbal communication, which may be useful for elucidating anxieties and treatment plans. Another disadvantage is that people may feel less comfortable communicating with a computer as opposed to a human. In a sexual history-taking setting in Australia using a computer-assisted self-interview, 51% of people were very comfortable with it, 35% were comfortable with it, and 14% were either uncomfortable or very uncomfortable with it.
The evidence for or against computer-assisted history taking systems is sparse. For example, as of 2011, there are no randomized control trials comparing computer-assisted versus traditional oral-and-written family history taking to identifying patients with an elevated risk of developing type 2 diabetes mellitus.