
Specialty gastroenterology ICD-9-CM 530.7 MedlinePlus 000269 | ICD-10 K22.6 DiseasesDB 7803 eMedicine ped/1359 | |
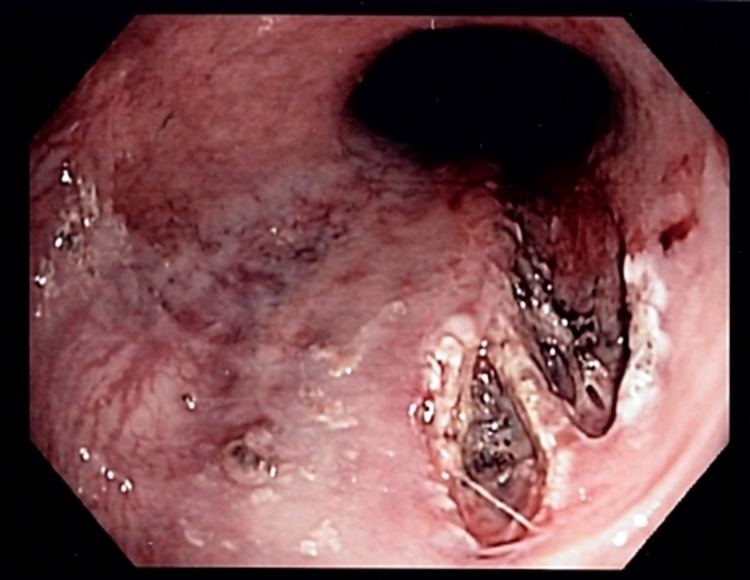 | ||
Mallory–Weiss syndrome or gastro-esophageal laceration syndrome refers to bleeding from a laceration in the mucosa at the junction of the stomach and esophagus. This is usually caused by severe vomiting because of alcoholism or bulimia, but can be caused by any conditions which causes violent vomiting and retching such as food poisoning. The syndrome presents with painless hematemesis. The laceration is sometimes referred to as a Mallory-Weiss tear.
Contents
Causes
It is often associated with alcoholism and eating disorders and there is some evidence that presence of a hiatal hernia is a predisposing condition. Forceful vomiting causes tear of the mucosa at the junction.
NSAID abuse is also a rare association. The tear involves mucosa and submucosa but not the muscular layer (contrast to Boerhaave syndrome which involves all the layers). The mean age is more than 60 and 80% are men. Hyperemesis gravidarum, which is severe morning sickness associated with vomiting and retching in pregnancy, is also a known cause of Mallory-Weiss tear.
Presentation
Mallory–Weiss syndrome often presents as an episode of vomiting up blood (hematemesis) after violent retching or vomiting, but may also be noticed as old blood in the stool (melena), and a history of retching may be absent.
In most cases, the bleeding stops spontaneously after 24–48 hours, but endoscopic or surgical treatment is sometimes required and rarely the condition is fatal. There won't be any abdominal pain.
Diagnosis
Definitive diagnosis is by endoscopy.
Treatment
Treatment is usually supportive as persistent bleeding is uncommon. However cauterization or injection of epinephrine to stop the bleeding may be undertaken during the index endoscopy procedure. Very rarely embolization of the arteries supplying the region may be required to stop the bleeding. If all other methods fail, high gastrostomy can be used to ligate the bleeding vessel. It is to be noted that the tube will not be able to stop bleeding as here the bleeding is arterial and the pressure in the balloon is not sufficient to overcome the arterial pressure.
History
The condition was first described in 1929 by G. Kenneth Mallory and Soma Weiss in 15 alcoholic patients.