
Latin macula lutea Dorlands
/Elsevier m_01/12509252 FMA 58637 | MeSH Macula+Lutea TA A15.2.04.021 | |
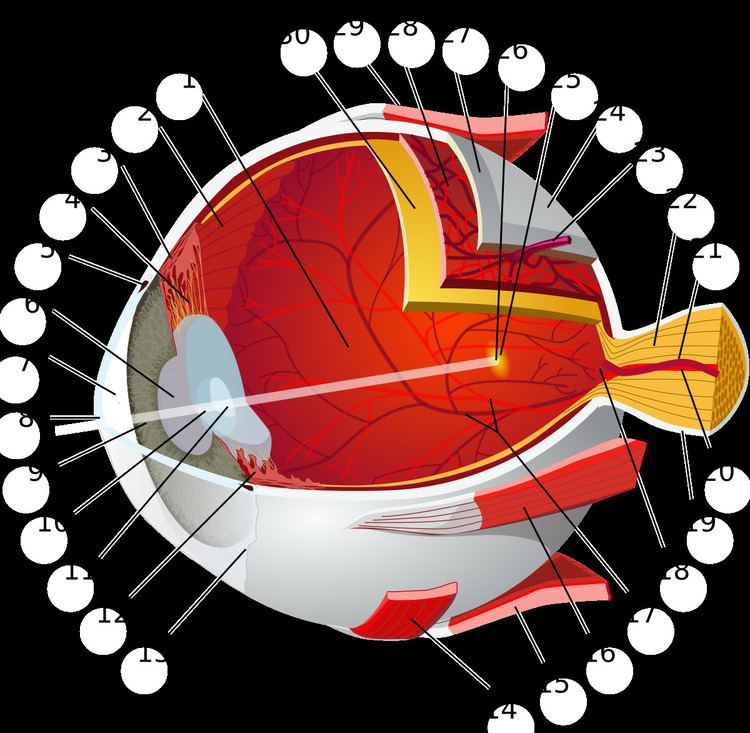 | ||
The macula or macula lutea (from Latin macula, "spot" + lutea, "yellow") is an oval-shaped pigmented area near the center of the retina of the human eye and some other animalian eyes. The macula in humans has a diameter of around 5.5 mm (0.22 in) and is subdivided into the umbo, foveola, foveal avascular zone (FAZ), fovea, parafovea, and perifovea areas. After death or enucleation (removal of the eye) the macula appears yellow, a color that is not visible in the living eye except when viewed with light from which red has been filtered. The anatomical macula at 5.5 mm (0.22 in) is much larger than the clinical macula which, at 1.5 mm (0.059 in), corresponds to the anatomical fovea. The clinical macula is seen when viewed from the pupil, as in ophthalmoscopy or retinal photography. The anatomical macula is defined histologically in terms of having two or more layers of ganglion cells. The umbo is the center of the foveola which in turn is located at the center of the fovea.
Contents
The fovea is located near the center of the macula. It is a small pit that contains the largest concentration of cone cells. The retina contains two types of photosensitive cells, the rod cells and the cones. The normal human eye contains three different types of cone, with different ranges of spectral sensitivity; hence the cones enable us to distinguish different colors. There is only one type of rod, but the rods are more sensitive than the cones, so in dim light we rely on them and do not discriminate colors. In the fovea centralis or macula lutea or simple yellow spot, cones predominate and are present at high density. The macula is thus responsible for the central, high-resolution, color vision that is possible in good light; and this kind of vision is impaired if the macula is damaged, for example in macular degeneration.
Color
Because the macula is yellow in colour it absorbs excess blue and ultraviolet light that enter the eye, and acts as a natural sunblock (analogous to sunglasses) for this area of the retina. The yellow color comes from its content of lutein and zeaxanthin, which are yellow xanthophyll carotenoids, derived from the diet. Zeaxanthin predominates at the macula, while lutein predominates elsewhere in the retina. There is some evidence that these carotenoids protect the pigmented region from some types of macular degeneration. A formulation of 10 mg lutein and 2 mg zeaxanthin has been shown to reduce the risk of age-related macular degeneration progressing to advanced stages, although these carotenoids have not been shown to prevent the disease.
Regions
Function
Structures in the macula are specialized for high-acuity vision. Within the macula are the fovea and foveola that both contain a high density of cones (photoreceptors with high acuity).
Clinical significance
Whereas loss of peripheral vision may go unnoticed for some time, damage to the macula will result in loss of central vision, which is usually immediately obvious. The progressive destruction of the macula is a disease known as macular degeneration and can sometimes lead to the creation of a macular hole. Macular holes are rarely caused by trauma, but if a severe blow is delivered it can burst the blood vessels going to the macula, destroying it.
Visual input from the macula occupies a substantial portion of the brain's visual capacity. As a result, some forms of visual field loss that occur without involving the macula are termed macular sparing. (For example, visual field testing might demonstrate homonymous hemianopsia with macular sparing.)
In the case of occipitoparietal ischemia owing to occlusion of elements of either posterior cerebral artery, patients may display cortical blindness (which, rarely, can involve blindness that the patient denies having, as seen in Anton's Syndrome), yet display sparing of the macula. This selective sparing is due to the collateral circulation offered to macular tracts by the middle cerebral artery. Neurological examination that confirms macular sparing can go far in representing the type of damage mediated by an infarct, in this case, indicating that the caudal visual cortex (which is the principal recipient of macular projections of the optic nerve) has been spared. Further, it indicates that cortical damage rostral to, and including, lateral geniculate nucleus is an unlikely outcome of the infarction, as too much of the lateral geniculate nucleus is, proportionally, devoted to macular-stream processing.