
Dorlands/Elsevier n_05/12566411 FMA 65296 | Innervates pectoralis major TA A14.2.03.018 | |
 | ||
Latin Nervus pectoralis lateralis | ||
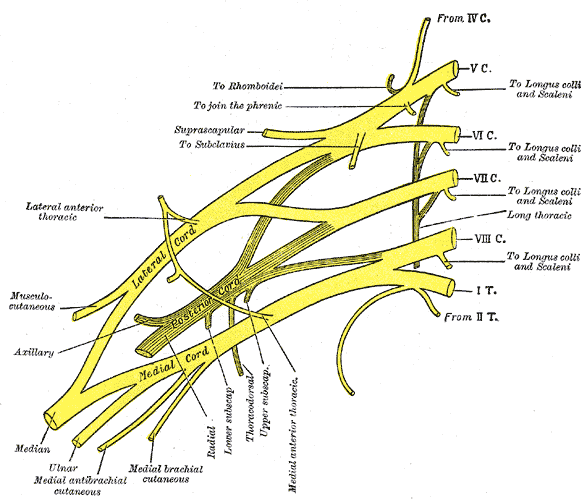
The lateral nerve (lateral anterior thoracic nerve) arises from the lateral cord of the brachial plexus, and through it from the fifth, sixth, and seventh cervical nerves.
Contents
It passes across the axillary artery and vein, pierces the clavipectoral (coracoclavicular) fascia, and is distributed to the deep surface of the Pectoralis major muscle.
Function
It sends a filament to join the medial (pectoral) anterior thoracic nerve and form with it a loop in front of the first part of the axillary artery.
Although this nerve is described as mostly motor, it also has been considered to carry proprioceptive and nociceptive fibers. It arises either from the lateral cord or directly from the anterior divisions of the upper and middle trunks of the brachial plexus, unlike the medial pectoral nerve, which derives from the medial cord (or directly from the anterior division of the lower trunk). It splits into four to seven branches that pierce the clavipectoral fascia to innervate the entire pectoralis major or its superior portion. The medial and lateral pectoral nerves form a connection, or loop, around the axillary artery, called ansa pectoralis. The lateral pectoral nerve has been described as double, while the medial pectoral nerve has been described as single.
Clinical significance
The lateral pectoral nerve is important in the pain response after breast augmentation and mastectomy, and especially in breast implant surgery, when the implant is inserted by the subpectoral route. The pectoral nerves can be anesthetized (blocked) intraoperatively by the surgeon under direct vision by three injections - one to block the medial pectoral nerve, the second to block the perforating branches of the medial pectoral nerve, and the third to block the lateral pectoral nerve. An ultrasound-guided pectoral nerve block can also be performed preventively before the operation by an anesthesiologist, experienced in regional anesthesia. It is safe and relies on ultrasound imaging to localize the pectoralis major and minor muscles, the presumed course of the pectoral nerves and the optimal spread of the local anesthetic.
Blockade of the lateral pectoral nerve is helpful in cases such as shoulder dislocation and other orthopedic procedures, involving the shoulder. Spasms of the pectoralis major muscle and resulting severe pain (acute or chronic) may be reduced by pectoral nerve block or neuromuscular relaxation. Decreasing the pectoral muscle tone intraoperatively by neuromuscular relaxation (paralytic agents) or by a nerve block (local anesthetic injection), can facilitate better cosmetic results during breast augmentation or post-mastectomy breast implantation. “The skin projection point of the neurovascular bundle (NVB) represents the denervation point (DP).” The NVB (thoracoacromial artery and vein, plus the lateral pectoral nerve) may be the guide for local anesthetic applications in order to achieve pectoral muscle denervation. “Routine botulinum toxin infiltration of the chest wall musculature at the time of mastectomy and immediate reconstruction…would paralyze the muscles and reduce the postoperative pain caused by muscle spasm.”