
Pronunciation /kwɑːʃiˈɔːrkər/ ICD-10 E40, E42 DiseasesDB 7211 | ICD-9-CM 260 MedlinePlus 001604 | |
 | ||
Kwashiorkor is a form of severe protein–energy malnutrition characterized by edema, irritability, ulcerating dermatoses, and an enlarged liver with fatty infiltrates. Sufficient calorie intake, but with insufficient protein consumption, distinguishes it from marasmus. Kwashiorkor cases occur in areas of famine or poor food supply. Cases in the developed world are rare.
Contents
Jamaican pediatrician Cicely Williams introduced the name into the medical community in a 1935 Lancet article, two years after she published the disease's first formal description in the Western medical literature. The name is derived from the Ga language of coastal Ghana, translated as "the sickness the baby gets when the new baby comes" or "the disease of the deposed child", and reflecting the development of the condition in an older child who has been weaned from the breast when a younger sibling comes. Breast milk contains proteins and amino acids vital to a child's growth. In at-risk populations, kwashiorkor may develop after a mother weans her child from breast milk, replacing it with a diet high in carbohydrates, especially sugar.
Signs and symptoms
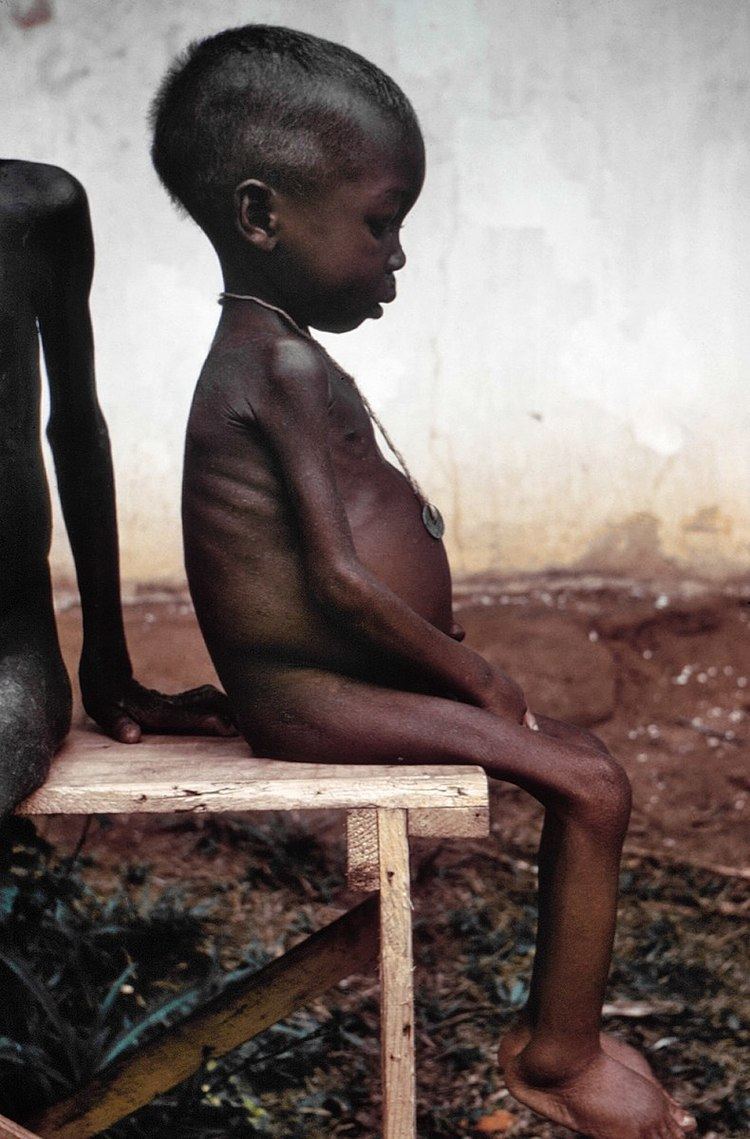
The defining sign of kwashiorkor in a malnourished child is pitting edema (swelling of the ankles and feet). Other signs include a distended abdomen, an enlarged liver with fatty infiltrates, thinning hair, loss of teeth, skin depigmentation and dermatitis. Children with kwashiorkor often develop irritability and anorexia. Generally, the disease can be treated by adding protein to the diet; however, it can have a long-term impact on a child's physical and mental development, and in severe cases may lead to death.
In dry climates, marasmus is the more frequent disease associated with malnutrition. Another malnutrition syndrome includes cachexia, although it is often caused by underlying illnesses. These are important considerations in the treatment of the patients.
Causes
Kwashiorkor is a severe form of malnutrition, caused by a deficiency in dietary protein. The extreme lack of protein causes an osmotic imbalance in the gastro-intestinal system causing swelling of the gut diagnosed as an edema or retention of water.
Extreme fluid retention observed in individuals suffering from kwashiorkor is a direct result of irregularities in the lymphatic system and an indication of capillary exchange. The lymphatic system serves three major purposes: fluid recovery, immunity, and lipid absorption. Victims of kwashiorkor commonly exhibit reduced ability to recover fluids, immune system failure, and low lipid absorption, all of which result from a state of severe undernourishment. Fluid recovery in the lymphatic system is accomplished by re-absorption of water and proteins which are then returned to the blood. Compromised fluid recovery results in the characteristic belly distension observed in highly malnourished children.
Capillary exchange between the lymphatic system and the bloodstream is stunted due to the inability of the body to effectively overcome the hydrostatic pressure gradient. Proteins, mainly albumin, are responsible for creating the colloid osmotic pressure (COP) observed in the blood and tissue fluids. The difference in the COP of the blood and tissue is called the oncotic pressure. The oncotic pressure is in direct opposition with the hydrostatic pressure and tends to draw water back into the capillary by osmosis. However, due to the lack of proteins, no substantial pressure gradient can be established to draw fluids from the tissue back into the blood stream. This results in the pooling of fluids, causing the swelling and distention of the abdomen.
The low protein intake leads to some specific signs: edema of the hands and feet, irritability, anorexia, a desquamative rash, hair discolouration, and a large fatty liver. The typical swollen abdomen is due to two causes: ascites because of hypoalbuminemia (low oncotic pressure), and enlarged fatty liver.
Ignorance of nutrition can be a cause. Dr. Latham, director of the Program in International Nutrition at Cornell University, along with Keith Rosenberg cited a case where parents who fed their child cassava failed to recognize malnutrition because of the edema caused by the syndrome and insisted the child was well-nourished despite the lack of dietary protein.
Protein should be supplied only for anabolic purposes. The catabolic needs should be satisfied with carbohydrate and fat. Protein catabolism involves the urea cycle, which is located in the liver and can easily overwhelm the capacity of an already damaged organ. The resulting liver failure can be fatal. This means in patients suffering from kwashiorkor, protein must be introduced back into the diet gradually. Clinical solutions include weaning the affected with milk products and increasing the intake of proteinaceous material to daily recommended amounts.
Prognosis
Disorders usually resolve after early treatment. If the treatment is delayed, the overall health of the child is improved but physical (reduced) and intellectual (mental disabilities) sequelae are feared. Without treatment or if treatment occurs too late, death is inevitable.
A high risk of death is identified by a brachial perimeter < 11 cm or by a weight-to-height threshold < -3 SD. In practice, malnourished children with edema are suffering from potentially life-threatening severe malnutrition.
Treatment
In order to avoid problems, the organism must be rehabilitated with small but frequent rations, given every two to four hours. During one week, the diet, hyperglucidic, is gradually enriched in protein as well as essential elements: sweet milk with mineral salts and vitamins. The diet may include lactases - so that children who have developed lactose intolerance can ingest dairy products - and antibiotics - to compensate for immunodeficiency. After two to three weeks, the milk is replaced by boiled cereals fortified with minerals and vitamins until its mass is at least 80% of normal weight. Traditional food can then be reintroduced. The child is considered healed when his mass reaches 85% of normal.