
Abbreviation ISAAC Extinction 2012 Chair Prof M.I. Asher | Formation 1991 Region served Global | |
 | ||
Main organ ISAAC Steering Committee | ||
The International Study of Asthma and Allergies in Childhood (ISAAC) was the largest collaborative epidemiological study of children in the world. ISAAC has measured the symptom prevalence of asthma, rhinitis and eczema in almost 2 million children in 105 countries. The aims of the ISAAC programme were to continue to measure symptom prevalence and severity of asthma, rhinitis and eczema in children, especially in developing countries where it had not been documented before; measure time trends in these conditions; identify major risk factors for asthma, rhinitis and eczema in all regions of the world; and to develop interventions to reduce the prevalence, mortality and burden of disease of asthma, rhinitis and eczema.
Contents
Risk Factors for asthma in children include: Babies born too early, born by C-section, Having Atopy, Allergens, Exposure to smoke and pollution, having a parent who has Asthma, and genetics.
The ISAAC Programme formally finished in December 2012. A new network to continue ISAAC's work in asthma The Global Asthma Network was founded in 2012 and will extend the work of ISAAC in the asthma field.
History
The International Study of Asthma and Allergies in Childhood was formed in 1991 to facilitate research into asthma, rhinitis and eczema by promoting a standardised methodology able to be used in diverse locations around the world.
ISAAC developed from a merging of two multinational collaborative projects each investigating variations in childhood asthma at the population level. These were an initiative from Auckland, New Zealand to conduct an international comparative study of asthma severity, and an initiative from Bochum, Germany to conduct an international study to monitor time trends and determinants of the prevalence of asthma and allergies in children.
ISAAC was a unique project investigating variations in the prevalence of these conditions at the population level and their potential causes. ISAAC attracted significant worldwide interest and large-scale participation, and became the largest worldwide collaborative research project ever undertaken in children resulting in a Guinness World Record. Since 1991, the ISAAC programme has involved 306 research centres in 105 countries with nearly 2 million children.
Organization
The ISAAC programme is led by an international Steering Committee of 26 scientists including clinicians, some from developing countries, which oversee all aspects of the programme. Many of the Steering Committee members also have positions on or are advisors to other international bodies. The Steering Committee meets yearly and the ISAAC Executive has a monthly telephone conference. As can be seen from the diagram, decisions from the Steering Committee are then passed from the Regional Coordinators to the National Coordinators, and then to the individual research centres. The International Data Centre receives data from the centres, as well as advising at all levels on methodology or other aspects of the programme.
Methodology
The ISAAC Steering Committee developed a standardised core questionnaire to measure symptom prevalence of asthma, rhinitis and eczema. These questionnaires were tested and validated to ensure they were standardised across populations and age groups, and suitable for international comparisons, in different geographical locations and languages. Using standardised guidelines, the questionnaires were translated into 53 languages and the correctness evaluated. ISAAC involved two age groups of children, 13-14 year olds, who self completed the questionnaire, and 6-7 year olds, in which the questionnaire was completed by the parents. Subjects were selected from randomly selected schools within a specified geographical area (or all schools) around each study centre. An asthma symptoms video questionnaire for the adolescents was optional. A sample size of 3000 per age group was used to give sufficient power to detect differences in severity of asthma (90% at a 1% significance level), and a high participation rate was a requirement.
ISAAC also developed tools to assist centers with the methodology, including manuals and guidelines for fieldworkers. The Phase One and Three manuals detail the development, scientific background, aims and methods of the ISAAC programme. These tools are all available from the International Data Centre, based at The University of Auckland, New Zealand, or from the ISAAC website (http://isaac.auckland.ac.nz).
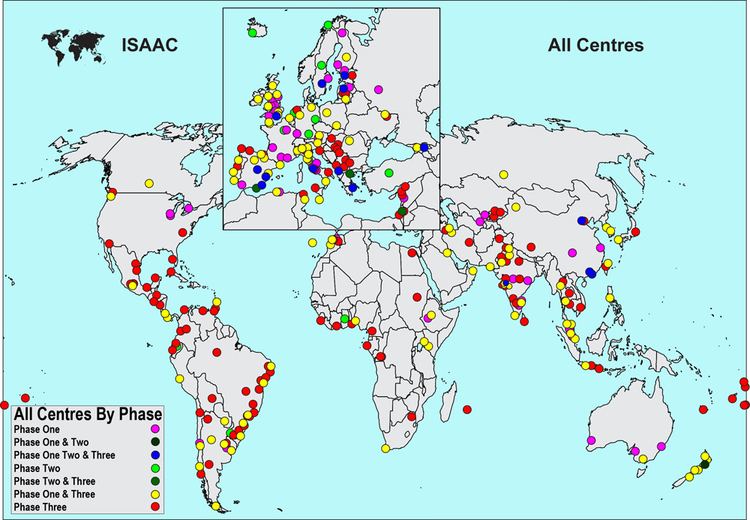
The collaborative studies were designed to be conducted in three phases. Phase One used the core questionnaires designed to assess the prevalence and severity of asthma and allergic disease in defined populations. Phase Two involved more intensive studies in a smaller number of selected centres and was designed to investigate the relative importance of hypotheses of interest that arose from the Phase One results. Phase Three was a repetition of Phase One, after at least five years, examining time trends in prevalences.
Phase One
ISAAC Phase One involved 156 collaborating centers in 56 countries with 721,601 participating children (3000 per age group per centre) and used the methodology described in the previous section. The aims of ISAAC Phase One were:
- To describe the prevalence and severity of asthma, rhinitis and eczema in children living in different centres and to make comparisons within and between countries;
- To obtain baseline measures for assessment of future trends in the prevalence and severity of these diseases; and
- To provide a framework for further aetiological research into lifestyle, environmental, genetic and medical care factors affecting these diseases.
Large variations in the symptom prevalence of asthma, rhinitis and eczema were found throughout the world mostly in hitherto unstudied populations. Reasons for these variations were explored with ecological analyses which identified possible protective factors as well as risk factors.
Phase Two
ISAAC Phase Two involved more intensive studies in a smaller number of selected centres. It began in 1998 and involved 30 centres in 22 countries with over 54,000 participating children. Phase Two was designed to investigate the relative importance of hypotheses of interest that arose from the Phase One results. ISAAC Phase Two enabled internationally standardised comparisons of disease and relevant risk factors using the modules developed by ISAAC collaborators (ISAAC Phase Two Modules Manual). These modules include the ISAAC core questionnaires, supplementary questionnaires, including questionnaires on disease management, child contact modules including examination for flexural dermatitis, skin prick tests for atopy, bronchial responsiveness to hypertonic saline, blood sampling and storage for serum IgE and genetic analyses, and a risk factor questionnaire module.
ISAAC Phase Two aims were:
- To describe the prevalence of 'objective' markers of asthma and allergies in children living in different centres, and to make comparisons within and between centres.
- To assess the relation between the prevalence of 'objective' markers of asthma and allergies and the prevalence of symptoms of these conditions in children living in different centres.
- To estimate to what extent the variation in the prevalence and severity of asthma and allergies in children between centres can be explained by differences in known or suspected risk factors or by differences in disease management.
Phase Two has shown little evidence of genetic factors in asthma and that most asthma, rhinitis and eczema has a non-allergic basis, especially in developing countries.
Phase Three
ISAAC Phase Three included many new centers from developing countries, with a total of 245 centers in 99 countries and 1,187,496 children being involved. ISAAC Phase Three repeated Phase One after at least five years for centres that undertook Phase One (time trends analyses). New centres which did not do Phase One (enlarged worldwide prevalence maps) were included, and an Environmental Questionnaire (EQ) was added. The EQ asked questions about diet, height, weight, heating and cooking fuels, exercise, pets, family size and birth order, socioeconomic status, immigration and tobacco smoke exposure. The specific aims of ISAAC Phase Three were:
- To examine time trends in the prevalence of asthma, allergic rhinitis atopic eczema in centres and countries which participated in ISAAC Phase One (Phase 3A centres).
- To describe the prevalence and severity of asthma, allergic rhinitis and atopic eczema in centres and countries which did not participate in Phase One (Phase 3B centres).
- To examine hypotheses at an individual level which have been suggested by the findings of Phase One, subsequent ecological analyses and recent advances in knowledge.
Phase Three identified major global variations in time trends and prevalence of childhood asthma, rhinitis and eczema. The EQ assessed the relationship between patterns found from the symptom prevalence data and many environmental factors. ISAAC Phase Three showed that in developing countries asthma and allergic disease were increasing, and risk factors that may have contributed to these increases are currently being analysed .
Phase Four
ISAAC Phase Four is the development and expansion of the scope of the ISAAC website (http://isaac.auckland.ac.nz) as a resource for ISAAC collaborators especially those in the developing world.
ISAAC was originally designed to have three phases; however, demand from researchers, particularly those in developing countries has indicated that a repeat cycle (Phase Five) is required. Funding is currently being sought to undertake this.
Impact
The ISAAC programme is currently the only global study of pediatric asthma and allergy currently in existence. Before ISAAC Phase Three, only five centres in the world had previously studied time trends in all three conditions. ISAAC Phase Three has provided time trend data in two age groups from 104 centres in 55 countries. ISAAC has established worldwide networks with organizations concerned with health in developing countries such as the International Union Against Tuberculosis and Lung Disease (IUATLD) and the World Health Organisation (WHO). Keys to ISAAC’s success have included the use of simple standardised questionnaires and rigorous data and methodology checks, to ensure standardised data that allows comparisons across geographic and linguistic boundaries.
ISAAC has demonstrated that asthma and allergies are a global health problem and environmental factors are key. The scientific value of ISAAC is attested to by the large number of publications produced by ISAAC collaborators, who have published more than 340 articles in over 100 journals including the Lancet, the British Medical Journal, the American Journal of Respiratory and Critical Care Medicine, Thorax and the European Respiratory Journal. The major effect of the findings has been to stimulate debates concerning the causes of the global variations in asthma, rhinitis and eczema, aided by the hypotheses suggested by the findings of the ecological analyses. ISAAC findings are cited by any organisation involved in monitoring and preventing Chronic Respiratory Diseases (CRD’s) and are used to inform Global Health Initiatives which include WHO, and its NGO (Non Governmental Organisation) the Global Alliance against Chronic Respiratory Diseases (GARD). ISAAC publications are included in the ‘GARD Basket’, a package of information, offered to countries by WHO to assist policy decisions relating to CRD’s.
In addition, the ISAAC Steering committee has successfully developed a surveillance tool that is able to be replicated in most places in the world, has enhanced research capacity into asthma and allergies throughout the world, and has been acknowledged for these roles by the WHO and the IUATLD – one of the leading bodies for respiratory health in developing countries. The ISAAC methodology has been the subject of positive editorial comment in the International Journal of Tuberculosis and Lung Disease, the official journal of the IUATLD, for its unique role in fostering research and critical thinking. They state “ISAAC is a model that should be followed by all those of us who are committed to improving public health in low-income countries.” ISAAC uses a simple framework which enables standard measures and comparisons across geographic, cultural and linguistic boundaries which means it can be carried out relatively inexpensively, making it particularly suitable for use in developing countries and allowing “truly global participation”. This inclusive and encouraging approach has resulted in ISAAC becoming the largest study of its kind. As stated by the Commission on Health Research for Development, ‘. . .for the world’s most vulnerable people, the benefits of research offer a potential for change that has gone largely untapped’. Such research is essential to improve public health globally and equitably. A major barrier to achieving this is a lack of confidence of health care workers to involve themselves in research. ISAAC has addressed this obstacle and produced a body of knowledge that informs policy. The World Allergy Organization has reported that “studies such as ISAAC are a major step toward overcoming barriers to the worldwide diagnosis and treatment of asthma”.
The ISA AC methodology has been adopted by the epidemiological community and is widely used in studies of asthma, rhinitis and eczema throughout the world.