
Type Intrauterine | Perfect use 0.2% | |
 | ||
First use 1990 (Mirena—currently available)
1976 (Progestasert—discontinued in 2001) Synonyms intrauterine system (IUS), levonorgestrel intrauterine system Trade names Kyleena, Liletta, Mirena, Skyla, others AHFS/Drugs.com Multum Consumer Information | ||
Intrauterine device (IUD) with progestogen, sold under the brand name Mirena among others, is a intrauterine device that releases the hormone levonorgestrel. It is used for birth control, heavy menstrual periods, and to prevent excessive build of the lining of the uterus in those on estrogen replacement therapy. It is one of the most effective forms of birth control with a one-year failure rate around 0.2%. The device is placed in the uterus and lasts three to five years. Following removal fertility returns quickly.
Contents
- Medical uses
- Effectiveness
- Breastfeeding
- Contraindications
- Side effects
- Cancer
- Bone density
- Composition and hormonal release
- Insertion and removal
- Mechanisms of action
- History
- Controversies
- References
Side effects include irregular periods, benign ovarian cysts, pelvic pain, and depression. Rarely uterine perforation may occur. Use is not recommended during pregnancy but is safe with breastfeeding. The IUD with progestogen is a type of long-acting reversible birth control. It works by making the mucous at the opening to the cervix thick, stopping the buildup of the lining of the uterus, and occasionally preventing ovulation.
The IUD with levonorgestrel was first approved for medical use in 1990 in Finland and in the United States in 2000. It is on the World Health Organization's List of Essential Medicines, the most effective and safe medicines needed in a health system. The wholesale cost in the developing world is about US$122.46 each. In the United Kingdom they cost the NHS about £88 pounds. In the United States they cost around US$844.00. More than 120 countries have approved the device and it is used by more than 10 million women.
Medical uses
In addition to birth control, hormonal IUD are used for prevention and treatment of:
Advantages
Disadvantages
Effectiveness
After insertion, Mirena is officially sold as effective for up to five years, although several studies have shown that it remains effective through seven years. Skyla is effective for 3 years.
The hormonal IUD is a long-acting reversible contraceptive, and is considered one of the most effective forms of birth control. The first year failure rate for the hormonal IUD is 0.2% and the five year failure rate is 0.7%. These rates are comparable to tubal sterilization, but unlike sterilization the effects of the hormonal IUD are reversible.
The hormonal IUD is considered to be more effective than other common forms of reversible contraception, such as the birth control pill, because it requires little action by the user after insertion. The effectiveness of other forms of birth control is mitigated (decreased) by the users themselves. If medication regimens for contraception are not followed precisely, the method becomes less effective. IUDs require no daily, weekly, or monthly regimen, so their typical use failure rate is therefore the same as their perfect use failure rate.
In women with bicornuate uterus and in need of contraception, two IUDs are generally applied (one in each horn) due to lack of evidence of efficacy with only one IUD. Evidence is lacking regarding progestogen IUD usage for menorrhagia in bicornuate uterus, but a case report showed good effect with a single IUD for this purpose.
Breastfeeding
Progestogen-only contraceptives such as an IUD are not believed to affect milk supply or infant growth. However, a study in the Mirena application for FDA approval found a lower continuation of breastfeeding at 75 days in hormonal IUD users (44%) versus copper IUD users (79%).
When using Mirena, about 0.1% of the maternal dose of levonorgestrel can be transferred via milk to the nursed infant. A six-year study of breastfed infants whose mothers used a levonorgestrel-only method of birth control found the infants had increased risk of respiratory infections and eye infections, though a lower risk of neurological conditions, compared to infants whose mothers used a copper IUD. No longer-term studies have been performed to assess the long-term effects on infants of levonorgestrel in breast milk.
There are conflicting recommendations about use of Mirena while breastfeeding. The U.S. FDA does not recommend any hormonal method, including Mirena, as a first choice of contraceptive for nursing mothers. The World Health Organization recommends against immediate postpartum insertion, citing increased expulsion rates. It also reports concerns about potential effects on the infant's liver and brain development in the first six weeks postpartum. However, it recommends offering Mirena as a contraceptive option beginning at six weeks postpartum even to nursing women. Planned Parenthood offers Mirena as a contraceptive option for breastfeeding women beginning at four weeks postpartum.
Contraindications
A hormonal IUD should not be used by women who:
Insertion of an IUD is not recommended for women having had a D&E abortion (second-trimester abortion) within the past four weeks. To reduce the risk of infection, insertion of an IUS is not recommended for women that have had a medical abortion but have not yet had an ultrasound to confirm that the abortion was complete, or that have not yet had their first menstruation following the medical abortion.
A full list of contraindications can be found in the WHO Medical Eligibility Criteria for Contraceptive Use and the CDCUnited States Medical Eligibility Criteria for Contraceptive Use.
Side effects
Cancer
According to a 1999 evaluation of the studies performed on progestin-only birth control by the International Agency for Research on Cancer, there is some evidence that progestin-only birth control reduces the risk of endometrial cancer. The IARC concluded that there is no evidence progestin-only birth control increases the risk of any cancer, though the available studies were too small to be definitively conclusive.
Progesterone is a hormone in the endometrium that counteracts estrogen driven growth. Very low levels of progesterone will cause estrogen to act more, leading to endometrial hyperplasia and adenocarcinoma. These effects can be minimized if treated with progestin, but not in very many cases.
Estrogen and progesterone have an antagonistic relationship. Estrogen promotes the growing of endometrial lining, while progesterone limits it. In the case of endometrial cancer, progesterone can negatively regulate estrogen driven growth. Tumors formed are correlated with insufficient progesterone and excess estrogen. In patients with endometrial cancer who use progestin releasing IUDs concluded mixed results.
Bone density
No evidence has been identified to suggest Mirena affects bone mineral density (BMD). Two small studies, limited to studying BMD in the forearm, show no decrease in BMD. One of the studies showed at 7 years of use, similar BMD at the midshaft of the ulna and at the distal radius as nonusers matched by age and BMI. In addition, BMD measurements were similar to the expected values for women in the same age group as the participants. The authors of the study said their results were predictable, since it is well established that the main factor responsible for bone loss in women is hypoestrogenism, and, in agreement with previous reports, they found estradiol levels in Mirena users to be normal.
Composition and hormonal release
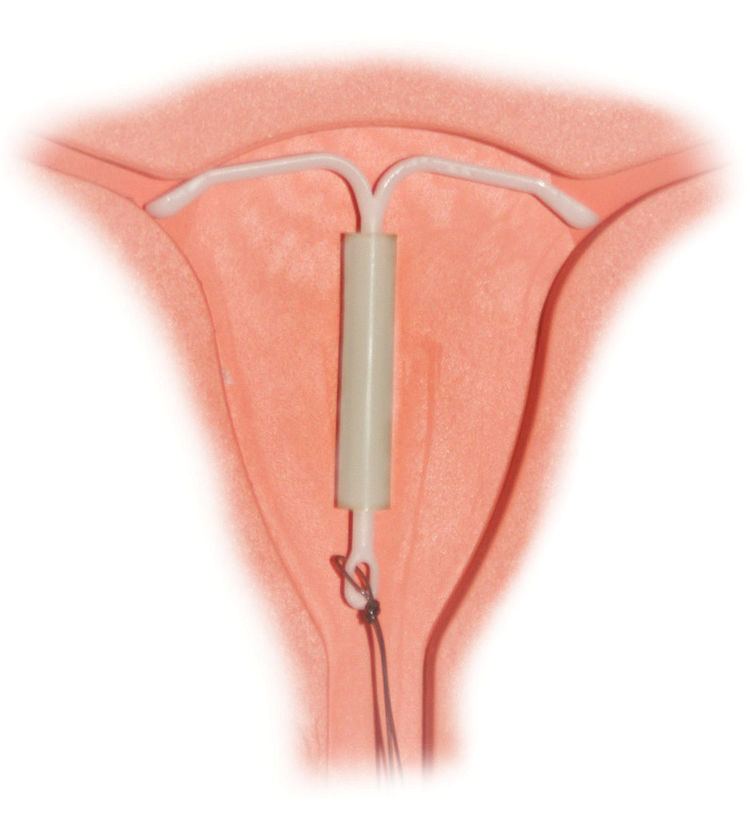
The hormonal IUD is a small 'T'-shaped piece of plastic, which contains levonorgestrel, a type of progestin. The cylinder of the device is coated with a membrane that regulates the release of the drug. Mirena releases the drug at an initial rate of 20 micrograms per day. This declines to a rate of 14 micrograms per day after 5 years, which is still in the range of clinical effectiveness. Skyla releases 14 micrograms per day and declines to 5 micrograms per day after 3 years. Bayer markets Skyla as Jaydess in the United Kingdom. Jaydess releases 6 micrograms per day and lasts for 3 years. In comparison, oral contraceptives can contain 150 micrograms of levonorgestrel. The hormonal IUD releases the levonorgestrel directly into the uterus, as such its effects are mostly paracrine rather than systemic. Most of the drug stays inside the uterus, and only a small amount is absorbed into the rest of the body. Blood levels of levonorgestrel in Mirena users are half those found in Norplant users and one-tenth those found in users of levonorgestrel-only pills).
Insertion and removal
The hormonal IUD is inserted in a similar procedure to the nonhormonal copper IUD, and can only be inserted by a qualified medical practitioner. Before insertion, a pelvic exam is performed to examine the shape and position of the uterus. It is also recommended that patients be tested for gonorrhea and chlamydia prior to insertion, as a current STI at the time of insertion can increase the risk of pelvic infection. During the insertion, the vagina is held open with a speculum, the same device used during a pap smear. A grasping instrument is used to steady the cervix, the length of the uterus is measured for proper insertion, and the IUD is placed using a narrow tube through the opening of the cervix into the uterus. A short length of monofilament plastic/nylon string hangs down from the cervix into the vagina. The string allows physicians and patients to check to ensure the IUD is still in place and enables easy removal of the device. Mild to moderate cramping can occur during the procedure, which generally takes five minutes or less. Insertion can be performed immediately postpartum and post-abortion if no infection has occurred. Misoprostol is not effective in reducing pain in IUD insertion.
Removal of the device should also be performed by a qualified medical practitioner. After removal, fertility will return to previous levels relatively quickly. One study found that the majority of participants returned to fertility within three months.
Mechanisms of action
The hormonal IUD's primary mechanism of action is to prevent fertilization. The levonorgestrel intrauterine system has several contraceptive effects:
Numerous studies have demonstrated that IUDs primarily prevent fertilization, not implantation. In one experiment involving tubal flushing, fertilized eggs were found in half of women not using contraception, but no fertilized eggs were found in women using IUDs. IUDs also decrease the risk of ectopic pregnancy, which further implies that IUDs prevent fertilization.
History
Hormonal IUDs were developed in the 1970s following the development of the copper IUD in the 1960s and 1970s. Dr. Antonio Scommenga, working at the Michael Reese Hospital in Chicago, discovered that administering progesterone inside the uterus could have contraceptive benefits. With knowledge of Scommegna's work, a Finnish doctor, Jouni Valtteri Tapani Luukkainen, created the 'T'-shaped IUD that released progesterone, marketed as the Progestasert System in 1976. This IUD had a short, 1-year lifespan and never achieved widespread popularity. Following this relative lack of success, Dr. Luukkainen replaced the progesterone with the hormone levonorgestrel to be released over a 5-year period, creating what is now Mirena.
The Mirena IUD was studied for safety and efficacy in two clinical trials in Finland and Sweden involving 1,169 women who were all between 18 and 35 years of age at the beginning of the trials. The trials included predominantly Caucasian women who had been previously pregnant with no history of ectopic pregnancy or pelvic inflammatory disease within the previous year. Over 70% of the participants had previously used IUDs.
In 2013 Skyla, a lower dose levonorgestrel IUD effective for up to 3 years, was approved by the FDA. Skyla has a different bleeding pattern than Mirena, with only 6% of women in clinical trials becoming amenorrheic (compared to approximately 20% with Mirena). In 2015, Liletta was approved by the FDA. Liletta has a similar size and levonorgestrel release characteristics as Mirena, and is FDA-approved for 3 years of use following a study in which 6 women out of 1,751 conceived while using Liletta.
Controversies
In 2009, Bayer, the maker of Mirena, was issued an FDA Warning Letter by the United States Food and Drug Administration for overstating the efficacy, minimizing the risks of use, and making "false or misleading presentations" about the device. From 2000 to 2013, the federal agency received over 70,072 complaints about the device and related adverse effects. As of April 2014, over 1,200 lawsuits have been filed in the United States.