
Group Group V ((−)ssRNA) Family Paramyxoviridae | Order Mononegavirales Genus Orthopneumovirus | |
 | ||
Species Human respiratory syncytial virus | ||
Human respiratory syncytial virus (HRSV) is a syncytial virus that causes respiratory tract infections. It is a major cause of lower respiratory tract infections and hospital visits during infancy and childhood. A prophylactic medication, palivizumab, can be employed to prevent HRSV in preterm (under 35 weeks gestation) infants, infants with certain congenital heart defects (CHD) or bronchopulmonary dysplasia (BPD), and infants with congenital malformations of the airway. Treatment is limited to supportive care (e.g. C-PAP), including oxygen therapy.
Contents
- Signs and symptoms
- Transmission
- Complications
- Taxonomy
- History
- Structure
- Genome
- Evolution
- Diagnosis
- Prevention
- Vaccine research
- Treatment
- References
In temperate climates there is an annual epidemic during the winter months. In tropical climates, infection is most common during the rainy season.
In the United States, 60% of infants are infected during their first HRSV season, and nearly all children will have been infected with the virus by 2–3 years of age. Of those infected with RSV, 2–3% will develop bronchiolitis, necessitating hospitalization. Natural infection with HRSV induces protective immunity which wanes over time—possibly more so than other respiratory viral infections—and thus people can be infected multiple times. Sometimes an infant can become symptomatically infected more than once, even within a single HRSV season. Severe HRSV infections have increasingly been found among elderly patients. Young adults can be re-infected every five to seven years, with symptoms looking like a sinus infection or a cold (infections can also be asymptomatic).
Signs and symptoms
The incubation time (from infection until symptoms arrive) is 4–5 days. For adults, HRSV produces mainly mild symptoms, often indistinguishable from common colds and minor illnesses. The Centers for Disease Control consider HRSV to be the "most common cause of bronchiolitis (inflammation of the small airways in the lung) and pneumonia in children under 1 year of age in the United States". For some children, RSV can cause bronchiolitis, leading to severe respiratory illness requiring hospitalization and, rarely, causing death. This is more likely to occur in patients that are immunocompromised or infants born prematurely. Other HRSV symptoms common among infants include listlessness, poor or diminished appetite, and a possible fever.
Recurrent wheezing and asthma are more common among individuals who suffered severe HRSV infection during the first few months of life than among controls; whether HRSV infection sets up a process that leads to recurrent wheezing or whether those already predisposed to asthma are more likely to become severely ill with HRSV has yet to be determined.
Symptoms of pneumonia in immuno-compromised patients such as in transplant patients and especially bone marrow transplant patients should be evaluated to rule out HRSV infection. This can be done by means of polymerase chain reaction (PCR) testing for HRSV nucleic acids in peripheral blood samples if all other infectious processes have been ruled out or if it is highly suspicious for RSV such as a recent exposure to a known source of HRSV infection.
In one case, HRSV onset appears to have coincided with the onset of type 2 diabetes.
Transmission
The incubation period is 2–8 days, but is usually 4–6 days.
HRSV spreads easily by direct contact, and can remain viable for a half an hour or more on hands or for up to 5 hours on countertops. Childcare facilities allow for rapid child-to-child transmission in a short period of time.
The HRSV is virtually the same as chimpanzee coryza virus and can be transmitted from apes to humans, although transmission from humans to apes is more common. The virus has also been recovered from cattle, goats and sheep, but these are not regarded as major vectors of transmission and there is no animal reservoir of the virus.
HRSV can last 2–8 days, but symptoms may persist for up to three weeks.
Complications
Taxonomy
HRSV is a negative-sense, single-stranded RNA virus of the family Pneumoviridae. Its name comes from the fact that F proteins on the surface of the virus cause the cell membranes on nearby cells to merge, forming syncytia.
History
HRSV was first isolated in 1956 from a chimpanzee called Chimpanzee Coryza Agent (CCA). Also in 1956, a new type of cytopathogenic myxovirus was isolated from a group of human infants with infantile croup.
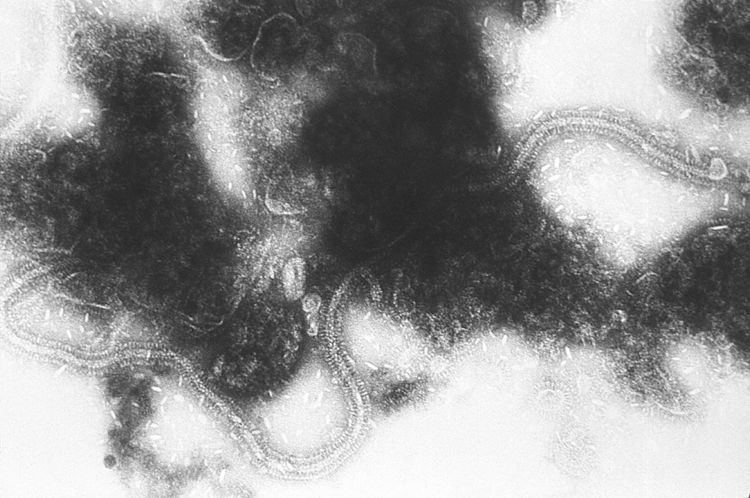
Structure
Human respiratory syncytial virus is a medium-sized (120-200 nm) enveloped virus that contains a lipoprotein coat and a linear negative-sense RNA genome (must be converted to an anti-sense genome prior to translation). The former contains virally encoded F, G, and SH lipoproteins. The F and G lipoproteins are the only two that target the cell membrane, and are highly conserved among RSV isolates. HRSV is divided into two antigenic subgroups, A and B, on the basis of the reactivity of the virus with monoclonal antibodies against the attachment (G) and fusion (F) glycoproteins. Subtype B is characterized as the asymptomatic strains of the virus that the majority of the population experiences. The more severe clinical illnesses involve subtype A strains, which tend to predominate in most outbreaks.
Four of the viral genes code for intracellular proteins that are involved in genome transcription, replication, and particle budding, namely N (nucleoprotein), P (phosphoprotein), M (matrix protein), and L (“large” protein, containing the RNA polymerase catalytic motifs). The RSV genomic RNA forms a helical ribonucleoprotein (RNP) complex with the N protein, termed nucleocapsid, which is used as template for RNA synthesis by the viral polymerase complex. The three-dimensional crystal structure of a decameric, annular ribonucleoprotein complex of the RSV nucleoprotein (N) bound to RNA has been determined at 3.3 Å resolution. This complex mimics one turn of the viral helical nucleocapsid complex. Its crystal structure was combined with electron microscopy data to provides a detailed model for the RSV nucleocapsid.
Genome
The genome is ~15,000 nucleotides in length and is composed of a single strand of RNA with negative polarity. It has 10 genes encoding 11 proteins.
To date, 10 HRSV-A genotypes have been designated, GA1 to GA7, SAA1, NA1, and NA2. The HRSV-B genotypes include GB1 to GB4, SAB1 to SAB3, and BA1 to BA6.
The genome of HRSV was completely sequenced in 1997.
Evolution
Bayesian estimates of the mutation rates in the subtype A genomes give a mutation rate of 6.47×10−4 (credible interval: 5.56×10−4 – 7.38×10−4) substitutions/site/year. This is similar to other RNA viruses. The population size has remained constant over the last 70 years and the G protein appears to be the main site of diversifying selection. The most recent common ancestor evolved ~1943 (credible interval: 1923–1954). The HRSV-B evolutionary rate (1.95×10−3 nucleotide substitutions/site/year) is similar to that previously estimated for HRSV-A (1.83×10−3 nucleotide substitutions/site/year). However, natural HRSV-B isolates appear to accommodate more drastic changes in their attachment G proteins. The most recent common ancestor of the currently circulating subgroup B strains was estimated to date back to around the year 1949. The divergence between the two major subgroups was calculated to have occurred approximately 350 years ago (mid-17th century).
Diagnosis
Human respiratory syncytial virus may be suspected based on the time of year of the infection; prevalence usually coincides with the winter flu season.
Several different types of laboratory tests are commercially available for diagnosis of RSV infection. Rapid diagnostic assays performed on respiratory specimens are available commercially. Most clinical laboratories currently utilize antigen detection tests. Compared with culture, the sensitivity of antigen detection tests generally ranges from 80% to 90%. Antigen detection tests and culture are generally reliable in young children but less useful in older children and adults.
Sensitivity of virus isolation from respiratory secretions in cell culture varies among laboratories. RT-PCR assays are now commercially available. The sensitivity of these assays is equal to or exceeds the sensitivity of virus isolation and antigen detections methods. Highly sensitive RT-PCR assays should be considered when testing adults, because they may have low viral loads in their respiratory specimens.
Serologic tests are less frequently used for diagnosis. Although useful for research, a diagnosis using a collection of paired acute and convalescent sera to demonstrate a significant rise in antibody titer to HRSV can not be made in time to guide care of the patient. On top of that, the antibody level does not always correlate with the acuteness or activity level of the infection.
RSV infection can be confirmed using tests for antigens or antibodies, or viral RNA by reverse transcription PCR. Quantification of viral load can be determined by various assay tests.
Prevention
As the virus is ubiquitous in all parts of the world, avoidance of infection is not possible.
However, palivizumab (brand name Synagis manufactured by MedImmune), a moderately effective prophylactic drug, is available for infants at high risk. Palivizumab is a monoclonal antibody directed against RSV surface fusion protein. It is given by monthly injections, which are begun just prior to the RSV season and are usually continued for five months. HRSV prophylaxis is indicated for infants that are premature or have either cardiac or lung disease, but the cost of prevention limits use in many parts of the world.
Vaccine research
A vaccine trial in 1960s using a formalin-inactivated vaccine (FI-RSV) increased disease severity in children who had been vaccinated. There is much active investigation into the development of a new vaccine, but at present no vaccine exists. Some of the most promising candidates are based on temperature sensitive mutants which have targeted genetic mutations to reduce virulence.
Scientists are attempting to develop a recombinant human respiratory syncytial virus vaccine that is suitable for intranasal instillation. Tests for determining the safety and level of resistance that can be achieved by the vaccine are being conducted in the chimpanzee, which is the only known animal that develops a respiratory illness similar to humans.
The development of a commercial HRSV vaccine has remained elusive. Recent breakthroughs have sparked continued interest in this highly sought after vaccine as the annual medical burden relating to HRSV has remained high, equal to Influenza and Pneumococcus.
On August 10, 2015, vaccine manufacturer Novavax announced Positive Top-Line Data from Phase 2 HRSV F-Protein Vaccine Clinical Trial in Older Adults. This was the first successful HRSV immunization Phase 2 trial for any population. On September 29, 2015, Novavax announced Positive Top-Line Data from Phase 2 Clinical Trial of RSV F Vaccine to Protect Infants via Maternal Immunization. These successive phase 2 accomplishments mark a significant turning point in the advancement towards an RSV vaccine.
On November 9, 2015, Novavax Initiated A Pivotal Phase 3 Trial of the HRSV F Vaccine in Older Adults and had fully enrolled this study on December 14, 2015. Top Line results released in Q3 of 2016 failed to prove that the vaccine was effective in preventing HRSV in older adults.
Treatment
To date, treatment has been limited to supportive measures. Adrenaline, bronchodilators, steroids, antibiotics, and ribavirin confer "no real benefit".
Studies of nebulized hypertonic saline have shown that the "use of nebulized 3% HS is a safe, inexpensive, and effective treatment for infants hospitalized with moderately severe viral bronchiolitis" where "respiratory syncytial virus (RSV) accounts for the majority of viral bronchiolitis cases". One study noted a 26% reduction in length of stay: 2.6 ± 1.9 days, compared with 3.5 ± 2.9 days in the normal-saline treated group (p=0.05).
Supportive care includes fluids and oxygen until the illness runs its course. Salbutamol may be used in an attempt to relieve any bronchospasm if present. Increased airflow, humidified and delivered via nasal cannula, may be supplied in order to reduce the effort required for respiration.