
ICD-10 C81 ICD-O 9650/3-9667/3 | ICD-9-CM 201 DiseasesDB 5973 | |
 | ||
Synonyms Hodgkin lymphoma, Hodgkin's disease Specialty Hematology and oncology | ||
Hodgkin's lymphoma (HL) is a type of lymphoma, which is generally believed to result from white blood cells of the lymphocyte kind. Symptoms may include fever, night sweats, and weight loss. Often there will be non-painful enlarged lymph nodes in the neck, under the arm, or in the groin. Those affected may feel tired or be itchy.
Contents
- Signs and symptoms
- Diagnosis
- Types
- Staging
- Pathology
- Management
- Adverse effects
- Prognosis
- Epidemiology
- UK
- History
- Notable cases
- References
About half of cases of Hodgkin's lymphoma are due to Epstein–Barr virus (EBV). Other risk factors include a family history of the condition and having HIV/AIDS. There are two major types of Hodgkin lymphoma: classical Hodgkin lymphoma and nodular lymphocyte-predominant Hodgkin lymphoma. Diagnosis is by finding Hodgkin's cells such as multinucleated Reed–Sternberg cells (RS cells) in lymph nodes.
Hodgkin lymphoma may be treated with chemotherapy, radiation therapy, and stem cell transplant. The choice of treatment often depends on how advanced the cancer is and whether or not it has favorable features. In early disease a cure is often possible. The percentage of people who survive five years in the United States is 86%. For those under the age of 20 rates of survival are 97%. Radiation and some chemotherapy drugs, however, increase the risk of other cancers, heart disease, or lung disease over the subsequent decades.
In 2013 about 725,000 people had Hodgkin's lymphoma and 24,000 died. In the United States 0.2% of people are affected at some point in their life. The most common age of diagnosis is between 20 and 40 years old. It was named after the English physician Thomas Hodgkin, who first described the condition in 1832.
Signs and symptoms
Patients with Hodgkin's lymphoma may present with the following symptoms:
Diagnosis
Hodgkin's lymphoma must be distinguished from non-cancerous causes of lymph node swelling (such as various infections) and from other types of cancer. Definitive diagnosis is by lymph node biopsy (usually excisional biopsy with microscopic examination). Blood tests are also performed to assess function of major organs and to assess safety for chemotherapy. Positron emission tomography (PET) is used to detect small deposits that do not show on CT scanning. PET scans are also useful in functional imaging (by using a radiolabeled glucose to image tissues of high metabolism). In some cases a Gallium Scan may be used instead of a PET scan.
Types
Classical Hodgkin lymphoma (excluding nodular lymphocyte predominant Hodgkin's lymphoma) can be subclassified into four pathologic subtypes based upon Reed–Sternberg cell morphology and the composition of the reactive cell infiltrate seen in the lymph node biopsy specimen (the cell composition around the Reed–Sternberg cell(s)).
Nodular lymphocyte predominant Hodgkin's lymphoma expresses CD20, and is not currently considered a form of classical Hodgkin's lymphoma.
For the other forms, although the traditional B-cell markers (such as CD20) are not expressed on all cells, Reed–Sternberg cells are usually of B cell origin. Although Hodgkin's is now frequently grouped with other B-cell malignancies, some T-cell markers (such as CD2 and CD4) are occasionally expressed. However, this may be an artifact of the ambiguity inherent in the diagnosis.
Hodgkin cells produce interleukin-21 (IL-21), which was once thought to be exclusive to T-cells. This feature may explain the behavior of classical Hodgkin's lymphoma, including clusters of other immune cells gathered around HL cells (infiltrate) in cultures.
Staging
The staging is the same for both Hodgkin's and non-Hodgkin's lymphomas.
After Hodgkin lymphoma is diagnosed, a patient will be staged: that is, they will undergo a series of tests and procedures that will determine what areas of the body are affected. These procedures may include documentation of their histology, a physical examination, blood tests, chest X-ray radiographs, computed tomography (CT)/Positron emission tomography (PET)/magnetic resonance imaging (MRI) scans of the chest, abdomen and pelvis, and usually a bone marrow biopsy. Positron emission tomography (PET) scan is now used instead of the gallium scan for staging. On the PET scan, sites involved with lymphoma light up very brightly enabling accurate and reproducible imaging. In the past, a lymphangiogram or surgical laparotomy (which involves opening the abdominal cavity and visually inspecting for tumors) were performed. Lymphangiograms or laparotomies are very rarely performed, having been supplanted by improvements in imaging with the CT scan and PET scan.
On the basis of this staging, the patient will be classified according to a staging classification (the Ann Arbor staging classification scheme is a common one):
The absence of systemic symptoms is signified by adding "A" to the stage; the presence of systemic symptoms is signified by adding "B" to the stage. For localised extranodal extension from mass of nodes that does not advance the stage, subscript "E" is added. Splenic involvement is signified by adding "S" to the stage. The inclusion of "bulky disease" is signified by "X".
Pathology
Affected lymph nodes (most often, laterocervical lymph nodes) are enlarged, but their shape is preserved because the capsule is not invaded. Usually, the cut surface is white-grey and uniform; in some histological subtypes (e.g. nodular sclerosis) a nodular aspect may appear.
A fibrin ring granuloma may be seen.
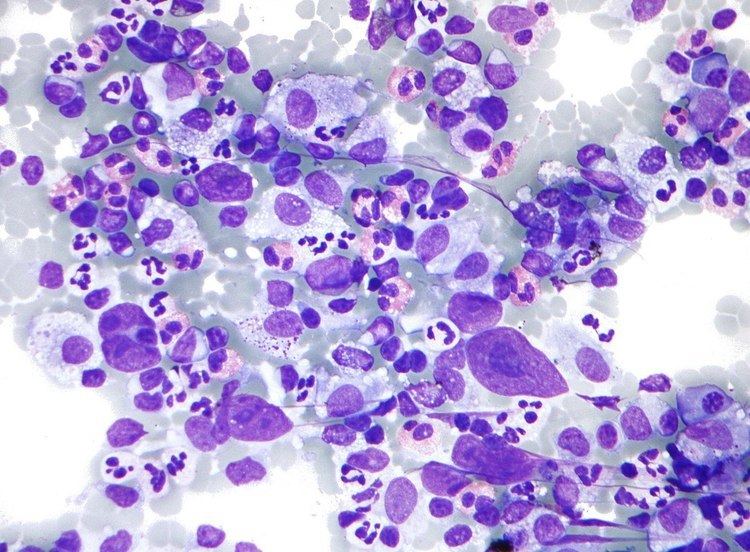
Microscopic examination of the lymph node biopsy reveals complete or partial effacement of the lymph node architecture by scattered large malignant cells known as Reed-Sternberg cells (RSC) (typical and variants) admixed within a reactive cell infiltrate composed of variable proportions of lymphocytes, histiocytes, eosinophils, and plasma cells. The Reed–Sternberg cells are identified as large often bi-nucleated cells with prominent nucleoli and an unusual CD45-, CD30+, CD15+/- immunophenotype. In approximately 50% of cases, the Reed–Sternberg cells are infected by the Epstein–Barr virus.
Characteristics of classic Reed–Sternberg cells include large size (20–50 micrometres), abundant, amphophilic, finely granular/homogeneous cytoplasm; two mirror-image nuclei (owl eyes) each with an eosinophilic nucleolus and a thick nuclear membrane (chromatin is distributed close to the nuclear membrane).
Variants:
Hodgkin's lymphoma can be sub-classified by histological type. The cell histology in Hodgkin's lymphoma is not as important as it is in non-Hodgkin's lymphoma: the treatment and prognosis in classic Hodgkin's lymphoma usually depends on the stage of disease rather than the histotype.
Management
Patients with early stage disease (IA or IIA) are effectively treated with radiation therapy or chemotherapy. The choice of treatment depends on the age, sex, bulk and the histological subtype of the disease. Adding localised radiation therapy after the chemotherapy regimen controls the tumors better and provides a better chance for survival than chemotherapy alone. Patients with later disease (III, IVA, or IVB) are treated with combination chemotherapy alone. Patients of any stage with a large mass in the chest are usually treated with combined chemotherapy and radiation therapy.
It should be noted that the common non-Hodgkin's treatment, rituximab (which is a monoclonal antibody against CD20) is not routinely used to treat Hodgkin's lymphoma due to the lack of CD20 surface antigens in most cases. The use of rituximab in Hodgkin's lymphoma, including the lymphocyte predominant subtype has been reviewed recently.
Although increased age is an adverse risk factor for Hodgkin's lymphoma, in general elderly patients without major comorbidities are sufficiently fit to tolerate standard therapy, and have a treatment outcome comparable to that of younger patients. However, the disease is a different entity in older patients and different considerations enter into treatment decisions.
For Hodgkin's lymphomas, radiation oncologists typically use external beam radiation therapy (sometimes shortened to EBRT or XRT). Radiation oncologists deliver external beam radiation therapy to the lymphoma from a machine called linear accelerator which produces high energy X Rays and Electrons. Patients usually describe treatments as painless and similar to getting an X-ray. Treatments last less than 30 minutes each.
For lymphomas, there are a few different ways radiation oncologists target the cancer cells. Involved field radiation is when the radiation oncologists give radiation only to those parts of the patient's body known to have the cancer. Very often, this is combined with chemotherapy. Radiation therapy directed above the diaphragm to the neck, chest and/or underarms is called mantle field radiation. Radiation to below the diaphragm to the abdomen, spleen and/or pelvis is called inverted-Y field radiation. Total nodal irradiation is when the therapist gives radiation to all the lymph nodes in the body to destroy cells that may have spread.
Adverse effects
The high cure rates and long survival of many patients with Hodgkin's lymphoma has led to a high concern with late adverse effects of treatment, including cardiovascular disease and second malignancies such as acute leukemias, lymphomas, and solid tumors within the radiation therapy field. Most patients with early-stage disease are now treated with abbreviated chemotherapy and involved-field radiation therapy rather than with radiation therapy alone. Clinical research strategies are exploring reduction of the duration of chemotherapy and dose and volume of radiation therapy in an attempt to reduce late morbidity and mortality of treatment while maintaining high cure rates. Hospitals are also treating those who respond quickly to chemotherapy with no radiation.
In childhood cases of Hodgkin's lymphoma, long-term endocrine adverse effects are a major concern, mainly gonadal dysfunction and growth retardation. Gonadal dysfunction seems to be the most severe endocrine long-term effect, especially after treatment with alkylating agents and/or pelvic radiotherapy.
Prognosis
Treatment of Hodgkin's disease has been improving over the past few decades. Recent trials that have made use of new types of chemotherapy have indicated higher survival rates than have previously been seen. In one recent European trial, the 5-year survival rate for those patients with a favorable prognosis was 98%, while that for patients with worse outlooks was at least 85%.
In 1998, an international effort identified seven prognostic factors that accurately predict the success rate of conventional treatment in patients with locally extensive or advanced stage Hodgkin's lymphoma. Freedom from progression (FFP) at 5 years was directly related to the number of factors present in a patient. The 5-year FFP for patients with zero factors is 84%. Each additional factor lowers the 5-year FFP rate by 7%, such that the 5-year FFP for a patient with 5 or more factors is 42%.
The adverse prognostic factors identified in the international study are:
Other studies have reported the following to be the most important adverse prognostic factors: mixed-cellularity or lymphocyte-depleted histologies, male sex, large number of involved nodal sites, advanced stage, age of 40 years or more, the presence of B symptoms, high erythrocyte sedimentation rate, and bulky disease (widening of the mediastinum by more than one third, or the presence of a nodal mass measuring more than 10 cm in any dimension.)
More recently, use of positron emission tomography (PET) early after commencing chemotherapy has demonstrated to have powerful prognostic ability. This enables assessment of an individual's response to chemotherapy as the PET activity switches off rapidly in patients who are responding. In this study, after two cycles of ABVD chemotherapy, 83% of patients were free of disease at 3 years if they had a negative PET versus only 28% in those with positive PET scans. This prognostic power exceeds conventional factors discussed above. Several trials are underway to see if PET-based risk adapted response can be used to improve patient outcomes by changing chemotherapy early in patients who are not responding.
Epidemiology
Unlike some other lymphomas, whose incidence increases with age, Hodgkin's lymphoma has a bimodal incidence curve; that is, it occurs most frequently in two separate age groups, the first being young adulthood (age 15–35) and the second being in those over 55 years old although these peaks may vary slightly with nationality. Overall, it is more common in males, except for the nodular sclerosis variant, which is slightly more common in females. The annual incidence of Hodgkin's lymphoma is 2.7 per 100,000 per persons per year, and the disease accounts for slightly less than 1% of all cancers worldwide.
In 2010, globally it resulted in about 18,000 deaths down from 19,000 in 1990.
The incidence of Hodgkin's lymphoma is increased in patients with HIV infection. In contrast to many other lymphomas associated with HIV infection it occurs most commonly in patients with higher CD4 T cell counts.
UK
Hodgkin lymphoma accounts for less than 1% of all cancer cases and deaths in the UK. Around 1,800 people were diagnosed with the disease in 2011, and around 330 people died in 2012.
History
Hodgkin's lymphoma was first described in an 1832 report by Thomas Hodgkin, although Hodgkin noted that perhaps the earliest reference to the condition was provided by Marcello Malpighi in 1666. While occupied as museum curator at Guy's Hospital, London, Hodgkin studied seven patients with painless lymph node enlargement. Of the seven cases, two were patients of Richard Bright, one was of Thomas Addison, and one was of Robert Carswell. Carswell's report of this seventh patient was accompanied by numerous illustrations that aided early descriptions of the disease.
Hodgkin's report on these seven patients, entitled "On some morbid appearances of the absorbent glands and spleen", was presented to the Medical and Chirurgical Society in London in January 1832 and was subsequently published in the society's journal, Medical-Chirurgical Society Transactions. Hodgkin's paper went largely unnoticed, however, even despite Bright highlighting it in an 1838 publication. Indeed, Hodgkin himself did not view his contribution as particularly significant.
In 1856, Samuel Wilks independently reported on a series of patients with the same disease that Hodgkin had previously described. Wilks, a successor to Hodgkin at Guy's Hospital, was unaware of Hodgkin's prior work on the subject. Bright made Wilks aware of Hodgkin's contribution and in 1865, Wilks published a second paper, entitled "Cases of enlargement of the lymphatic glands and spleen", in which he called the disease "Hodgkin's disease" in honor of his predecessor.
Theodor Langhans and WS Greenfield first described the microscopic characteristics of Hodgkin's lymphoma in 1872 and 1878, respectively. In 1898 and 1902, respectively, Carl Sternberg and Dorothy Reed independently described the cytogenetic features of the malignant cells of Hodgkin's lymphoma, now called Reed–Sternberg cells.
Tissue specimens from Hodgkin's seven patients remained at Guy's Hospital for a number of years. Nearly 100 years after Hodgkin's initial publication, histopathologic reexamination confirmed Hodgkin's lymphoma in only three of seven of these patients. The remaining cases included non-Hodgkin lymphoma, tuberculosis, and syphilis.
Hodgkin's lymphoma was one of the first cancers which could be treated using radiation therapy and, later, it was one of the first to be treated by combination chemotherapy.