
 | ||
Health care reform in the United States has a long history. Reforms have often been proposed but have rarely been accomplished. In 2010, landmark reform was passed through two federal statutes enacted in 2010: the Patient Protection and Affordable Care Act (PPACA), signed March 23, 2010, and the Health Care and Education Reconciliation Act of 2010 (H
Contents
- History of national reform efforts
- Motivation
- Insurance cost and availability
- Waste and fraud
- Quality of care
- Public opinion
- Patient Protection and Affordable Care Act
- Alternatives and research directions
- Single payer health care
- Public option
- Balancing doctor supply and demand
- Bundled payments
- Trump administration efforts
- References
Future reforms of the American health care system continue to be proposed, with notable proposals including a single-payer system and a reduction in fee-for-service medical care. The PPACA includes a new agency, the Center for Medicare and Medicaid Innovation, which is intended to research reform ideas through pilot projects.
History of national reform efforts
Here is a summary of reform achievements at the national level in the United States. For failed efforts, state-based efforts, native tribes services and more details generally, see the main article History of health care reform in the United States.
Motivation
International comparisons of healthcare have found that the United States spends more per-capita than other similarly developed nations but falls below similar countries in various health metrics, suggesting inefficiency and waste. In addition, the United States has significant underinsurance and significant impending unfunded liabilities from its aging demographic and its social insurance programs Medicare and Medicaid (Medicaid provides free long-term care to the elderly poor). The fiscal and human impact of these issues have motivated reform proposals.
According to 2009 World Bank statistics, the U.S. had the highest healthcare costs relative to the size of the economy (GDP) in the world, even though estimated 50 million citizens (approximately 16% of the September 2011 estimated population of 312 million) lacked insurance. In March 2010, billionaire Warren Buffett commented that the high costs paid by U.S. companies for their employees' health care put them at a competitive disadvantage.
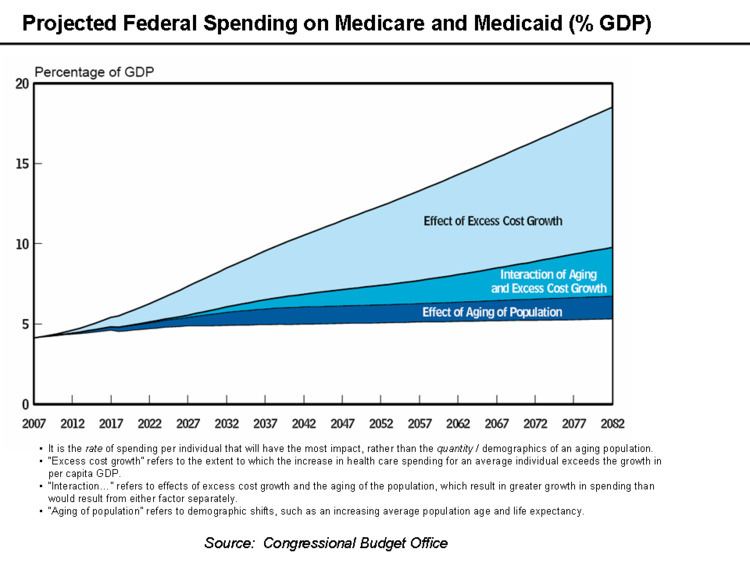
Further, an estimated 77 million Baby Boomers are reaching retirement age, which combined with significant annual increases in healthcare costs per person will place enormous budgetary strain on U.S. state and federal governments, particularly through Medicare and Medicaid spending (Medicaid provides long-term care for the elderly poor). Maintaining the long-term fiscal health of the U.S. federal government is significantly dependent on healthcare costs being controlled.
Insurance cost and availability
In addition, the number of employers who offer health insurance has declined and costs for employer-paid health insurance are rising: from 2001 to 2007, premiums for family coverage increased 78%, while wages rose 19% and prices rose 17%, according to the Kaiser Family Foundation. Even for those who are employed, the private insurance in the US varies greatly in its coverage; one study by the Commonwealth Fund published in Health Affairs estimated that 16 million U.S. adults were underinsured in 2003. The underinsured were significantly more likely than those with adequate insurance to forgo health care, report financial stress because of medical bills, and experience coverage gaps for such items as prescription drugs. The study found that underinsurance disproportionately affects those with lower incomes—73% of the underinsured in the study population had annual incomes below 200% of the federal poverty level. However, a study published by the Kaiser Family Foundation in 2008 found that the typical large employer preferred provider organization (PPO) plan in 2007 was more generous than either Medicare or the Federal Employees Health Benefits Program Standard Option. One indicator of the consequences of Americans' inconsistent health care coverage is a study in Health Affairs that concluded that half of personal bankruptcys involved medical bills, although other sources dispute this.
There are health losses from insufficient health insurance. A 2009 Harvard study published in the American Journal of Public Health found more than 44,800 excess deaths annually in the United States due to Americans lacking health insurance. More broadly, estimates of the total number of people in the United States, whether insured or uninsured, who die because of lack of medical care were estimated in a 1997 analysis to be nearly 100,000 per year. A study of the effects of the Massachusetts universal health care law (which took effect in 2006) found a 3% drop in mortality among people 20–64 years old—1 death per 830 people with insurance. Other studies, just as those examining the randomized distribution of Medicaid insurance to low-income people in Oregon in 2008, found no change in death rate.
The cost of insurance has been a primary motivation in the reform of the US healthcare system, and many different explanations have been proposed in the reasons for high insurance costs and how to remedy them. One critique and motivation for healthcare reform has been the development of the medical–industrial complex. This relates to moral arguments for health care reform, framing healthcare as a social good, one that is fundamentally immoral to deny to people based on economic status. The motivation behind healthcare reform in response to the medical-industrial complex also stems from issues of social inequity, promotion of medicine over preventative care. The medical-industrial complex, defined as a network of health insurance companies, pharmaceutical companies, and the like, plays a role in the complexity of the US insurance market and a fine line between government and industry within it. Likewise, critiques of insurance markets being conducted under a capitalistic, free-market model also include that medical solutions, as opposed to preventative healthcare measures, are promoted to maintain this medical-industrial complex. Arguments for a market-based approach to health insurance include the Grossman model, which is based on an ideal competitive model, but others have critiqued this, arguing that fundamentally, this means that people in higher socioeconomic levels will receive a better quality of healthcare.
Another concern is the rate of uninsured people in the US. In June 2014, Gallup–Healthways Well–Being conducted a survey and found that the uninsured rate is going down. 13 percent of U.S. adults are uninsured in 2014. This is a decrease from the percentage at 17 percent in January 2014 and translates to roughly 10 million to 11 million individuals who gained coverage. The survey also looked at the major demographic groups and found each is making progress towards getting health insurance. However, Hispanics, who have the highest uninsured rate of any racial or ethnic group, are lagging in their progress. Under the new health care reform, Latinos were expected to be major beneficiaries of the new health care law. Gallup found that the biggest drop in the uninsured rate (3 percentage points) was among households making less than $36,000 a year.
Waste and fraud
In December 2011 the outgoing Administrator of the Centers for Medicare & Medicaid Services, Donald Berwick, asserted that 20% to 30% of health care spending is waste. He listed five causes for the waste: (1) overtreatment of patients, (2) the failure to coordinate care, (3) the administrative complexity of the health care system, (4) burdensome rules and (5) fraud.
An estimated 3–10% of all health care expenditures in the U.S. are fraudulent. In 2011, Medicare and Medicaid made $65 billion in improper payments (including both error and fraud). Government efforts to reduce fraud include $4 billion in fraudulent payments recovered by the Department of Justice and the FBI in 2012, longer jail sentences specified by the Affordable Care Act, and Senior Medicare Patrols—volunteers trained to identify and report fraud.
In 2007, the Department of Justice and Health and Human Services formed the Medicare Fraud Strike Force to combat fraud through data analysis and increased community policing. As of May 2013, the Strike Force has charged more than 1,500 people for false billings of more than $5 billion. Medicare fraud often takes the form of kickbacks and money-laundering. Fraud schemes often take the form of billing for medically unnecessary services or services not rendered.
Quality of care
There is significant debate regarding the quality of the U.S. healthcare system relative to those of other countries. Physicians for a National Health Program, a political advocacy group, has claimed that a free market solution to health care provides a lower quality of care, with higher mortality rates, than publicly funded systems. The quality of health maintenance organizations and managed care have also been criticized by this same group.
According to a 2000 study of the World Health Organization, publicly funded systems of industrial nations spend less on health care, both as a percentage of their GDP and per capita, and enjoy superior population-based health care outcomes. However, conservative commentator David Gratzer and the Cato Institute, a libertarian think tank, have both criticized the WHO's comparison method for being biased; the WHO study marked down countries for having private or fee-paying health treatment and rated countries by comparison to their expected health care performance, rather than objectively comparing quality of care.
Some medical researchers say that patient satisfaction surveys are a poor way to evaluate medical care. Researchers at the RAND Corporation and the Department of Veterans Affairs asked 236 elderly patients in two different managed care plans to rate their care, then examined care in medical records, as reported in Annals of Internal Medicine. There was no correlation. "Patient ratings of health care are easy to obtain and report, but do not accurately measure the technical quality of medical care," said John T. Chang, UCLA, lead author.
Public opinion
Public opinion polls have shown a majority of the public supports various levels of government involvement in health care in the United States, with stated preferences depending on how the question is asked. Polls from Harvard University in 1988, the Los Angeles Times in 1990, and the Wall Street Journal in 1991 all showed strong support for a health care system compared to the system in Canada. More recently, however, polling support has declined for that sort of health care system, with a 2007 Yahoo/AP poll showing a majority of respondents considered themselves supporters of "single-payer health care," a majority in favor of a number of reforms according to a joint poll with the Los Angeles Times and Bloomberg, and a plurality of respondents in a 2009 poll for Time Magazine showed support for "a national single-payer plan similar to Medicare for all." Polls by Rasmussen Reports in 2011 and 2012 showed pluralities opposed to single-payer health care. Many other polls show support for various levels of government involvement in health care, including polls from New York Times/CBS News and Washington Post/ABC News, showing favorability for a form of national health insurance. The Kaiser Family Foundation showed a majority in favor of a form of national health insurance, often compared to Medicare, and a Quinnipiac poll in three states in 2008 found majority support for the government ensuring "that everyone in the United States has adequate health-care" among likely Democratic primary voters.
A 2001 article in the public health journal Health Affairs studied fifty years of American public opinion of various health care plans and concluded that, while there appears to be general support of a "national health care plan," poll respondents "remain satisfied with their current medical arrangements, do not trust the federal government to do what is right, and do not favor a single-payer type of national health plan." Politifact rated a statement by Michael Moore "false" when he stated that "[t]he majority actually want single-payer health care." According to Politifact, responses on these polls largely depend on the wording. For example, people respond more favorably when they are asked if they want a system "like Medicare".
Patient Protection and Affordable Care Act
After campaigning on the promise of health care reform, President Barack Obama gave a speech in March 2010 at a rally in Pennsylvania explaining the necessity of health insurance reform and calling on Congress to hold a final up or down vote on reform. The result of his efforts was the Patient Protection and Affordable Care Act. Because Obama's party did not have a filibuster-proof majority in the Senate, the law was amended by the Health Care and Education Reconciliation Act of 2010 using the reconciliation process in which debate in the Senate is limited and the filibuster is therefore not permitted.
The legislation remains controversial, with some states challenging it in federal court and opposition from some voters. In June 2012, in a 5–4 decision, the U.S. Supreme Court found major portions of the law to be constitutional. However, the law continues to face legal challenges. The latest attempt at reversing the Affordable Care Act occurred during the Government Shutdown on October 1, 2013. Government officials that oppose the ACA tried to make approval of a bill to reopen the government contingent on the demise of the ACA. This attempt met with failure and the government reopened on November 16, 2013.
As a result of the law, insurance companies can no longer charge members based on gender, burdening men with the health care costs of women. A study by the National Institutes of Health reported that the lifetime per capita expenditure at birth, using year 2000 dollars, showed a large difference between health care costs of females ($361,192) and males ($268,679). A large portion of this cost difference is in the shorter lifespan of men, but even after adjustment for age (assume men live as long as women), there still is a 20% difference in lifetime health care expenditures.
The act's provisions become effective over time. The most significant changes, particularly affecting the availability and terms of insurance become effective January 1, 2014. These include an expansion of Medicaid (at the option of each state) to those without dependent children and subsidized healthcare exchanges. Changes which occur earlier include allowing dependents to remain on their plan until 26, limitations on rescission (dropping insureds when they get sick), removal of lifetime coverage limits, mandates that insurers fully cover certain preventative services, high-risk pools for uninsureds, tax credits for businesses to provide insurance to employees, an insurance company rate review program, and minimum medical loss ratios.
The law creates the Patient-Centered Outcomes Research Institute to study comparative effectiveness research funded by a fee on insurers per covered life (starting at $1, increasing to $2 and thereafter adjusted according to an index). It also allowed the FDA to approve generic biologic drugs and specifically allows for 12 years of exclusive use for newly developed biologic drugs.
In addition, the law explores some programs intended to increase incentives to provide quality and collaborative care, such as accountable care organizations. The Center for Medicare and Medicaid Innovation was created to fund pilot programs which may reduce costs; the experiments cover nearly every idea healthcare experts advocate, except malpractice/tort reform. The law also requires for reduced Medicare reimbursements for hospitals with excess readmissions and eventually ties physician Medicare reimbursements to quality of care metrics.
The law is also designed to complement the 2009 HITECH Act which encourages the "meaningful use" of electronic health records; for example, the law directs the government to make use of these records for analyzing healthcare provider quality.
The Affordable Care Act also aims to promote access to preventative healthcare. Through providing access to screenings for diseases like breast cancer, promoting health in the workplace, and community preventative health, the Affordable Care Act contains sections that advance and promote preventative health initiatives.
Alternatives and research directions
There are alternatives to the exchange-based market system which was enacted by the Patient Protection and Affordable Care Act which have been proposed in the past and continue to be proposed, such as a single-payer system and allowing health insurance to be regulated at the federal level.
In addition, the Patient Protection and Affordable Health Care Act of 2010 contained provisions which allows the Centers for Medicare and Medicaid Services (CMS) to undertake pilot projects which, if they are successful could be implemented in future.
Single-payer health care
A number of proposals have been made for a universal single-payer healthcare system in the United States, most recently the United States National Health Care Act, (popularly known as H.R. 676 or "Medicare for All") but none have achieved more political support than 20% congressional co-sponsorship. Advocates argue that preventative health care expenditures can save several hundreds of billions of dollars per year because publicly funded universal health care would benefit employers and consumers, that employers would benefit from a bigger pool of potential customers and that employers would likely pay less, and would be spared administrative costs of health care benefits. It is also argued that inequities between employers would be reduced. Also, for example, cancer patients are more likely to be diagnosed at Stage I where curative treatment is typically a few outpatient visits, instead of at Stage III or later in an emergency room where treatment can involve years of hospitalization and is often terminal. Others have estimated a long-term savings amounting to 40% of all national health expenditures due to preventative health care, although estimates from the Congressional Budget Office and The New England Journal of Medicine have found that preventative care is more expensive.
Any national system would be paid for in part through taxes replacing insurance premiums, but advocates also believe savings would be realized through preventative care and the elimination of insurance company overhead and hospital billing costs. An analysis of a single-payer bill by Physicians for a National Health Program estimated the immediate savings at $350 billion per year. The Commonwealth Fund believes that, if the United States adopted a universal health care system, the mortality rate would improve and the country would save approximately $570 billion a year.
Recent enactments of single-payer systems within individual states, such as in Vermont in 2011, may serve as living models supporting federal single-payer coverage. The plan in Vermont, however, has failed.
Public option
In January 2013, Representative Jan Schakowsky and 44 other U.S. House of Representatives Democrats introduced H
Balancing doctor supply and demand
The Medicare Graduate Medical Education program regulates the supply of medical doctors in the U.S. By adjusting the reimbursement rates to establish more income equality among the medical professions, the effective cost of medical care can be lowered.
Bundled payments
A key project is one that could radically change the way the medical profession is paid for services under Medicare and Medicaid. The current system, which is also the prime system used by medical insurers is known as fee-for-service because the medical practitioner is paid only for the performance of medical procedures which, it is argued means that doctors have a financial incentive to do more tests (which generates more income) which may not be in the patients' best long-term interest. The current system encourages medical interventions such as surgeries and prescribed medicines (all of which carry some risk for the patient but increase revenues for the medical care industry) and does not reward other activities such as encouraging behavioral changes such as modifying dietary habits and quitting smoking, or follow-ups regarding prescribed regimes which could have better outcomes for the patient at a lower cost. The current fee-for-service system also rewards bad hospitals for bad service. Some have noted that the best hospitals have fewer re-admission rates than others, which benefits patients, but some of the worst hospitals have high re-admission rates which is bad for patients but is perversely rewarded under the fee-for-service system.
Projects at CMS are examining the possibility of rewarding health care providers through a process known as "bundled payments" by which local doctors and hospitals in an area would be paid not on a fee for service basis but on a capitation system linked to outcomes. The areas with the best outcomes would get more. This system, it is argued, makes medical practitioners much more concerned to focus on activities that deliver real health benefits at a lower cost to the system by removing the perversities inherent in the fee-for-service system.
Though aimed as a model for health care funded by CMS, if the project is successful it is thought that the model could be followed by the commercial health insurance industry also.
Trump administration efforts
Donald Trump was elected President on a platform that included a pledge to "repeal and replace" the Patient Protection and Affordable Care Act (commonly called the Affordable Care Act or Obamacare). To that end it is supporting the proposed American Health Care Act (ACHA), developed by the House of Representatives. The administration has suggested that the ACHA is only part of its reform efforts. Other proposals include allowing interstate competition in the health insurance market.