
 | ||
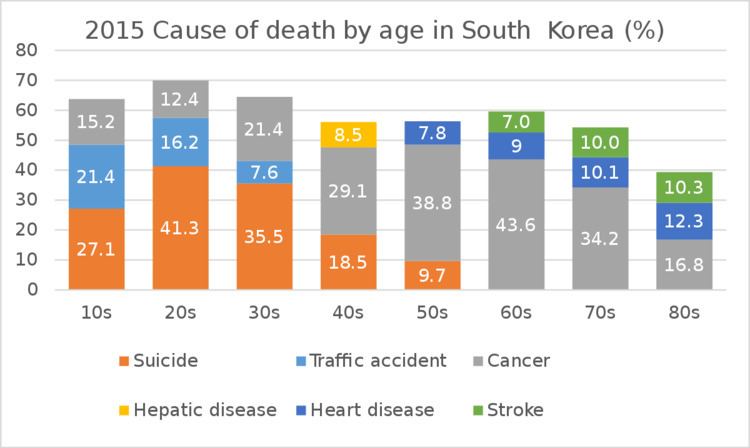
South Korea has the 11th-highest life expectancy in the world and the second-least obese rate in the OECD. The male smoking rate is 49.8% (female 4.2%). Suicide in South Korea is a serious and widespread problem. The suicide rate is the highest in the OECD in 2012 (29.1 deaths per 100,000 persons). Additionally, South Korea's suicide rate is also ranked the highest in the world in 2012 according to WHO data (36.8 deaths per 100,000 persons).
Contents
- Health insurance system
- Hospitals
- Drinking alcohol
- Air pollution
- Chronic disease
- Unequal distribution of physicians
- References
South Korea maintains a universal healthcare system that is rated as the fourth most efficient healthcare system out of the 55 nations rated as of 2016 after Hong Kong, Singapore and Spain by Bloomberg.
Health insurance system
Social health insurance was introduced with the 1977 National Health Insurance Act, which provided industrial workers in large corporations with health insurance. The program was expanded in 1979 to include other workers, such as government employees and private teachers. This program was thereafter progressively rolled out to the general public, finally achieving universal coverage in 1989. Despite being able to achieve universal health care, this program resulted in more equity issues within society as it grouped people into different categories based on demographic factors like geographical location and employment type. These different groups ultimately received different coverage from their respective healthcare providers.
The healthcare system was initially reliant on not-for-profit insurance societies to manage and provide the health insurance coverage. As the program expanded from 1977 to 1989, the government decided to allow different insurance societies to provide coverage for different sections of the population in order to minimize government intervention in the health insurance system. This eventually produced a very inefficient system, which resulted in more than 350 different health insurance societies. A major healthcare financing reform in 2000 merged all medical societies into the National Health Insurance Service. This new service became a single-payer healthcare system in 2004. The four-year delay occurred because of disagreements in the legislature on how to properly assess self-employed individuals in order to determine their contribution.
The insurance system is funded by contributions, government subsidies, and tobacco surcharges and the National Health Insurance Corporation is the main supervising institution. Employed contributors are expected to pay 5.08% of their income while self-employed contributions are calculated based on the income and property of the individual. The national government provides 14% of the total amount of funding and the tobacco surcharges account for 6% of the funding. The total expenditure on health insurance as a percentage of gross domestic product has increased from 4.0% in 2000 to 7.1% in 2014. In 2014, total health expenditure per capita was $2,531, compared to a global average of $1058, and government expenditure on health per capita was $1368.
Hospitals
The number of hospital beds per 1000 population is 10, well above the OECD countries' average of 5. According to Mark Britnell hospitals dominate the health system. 94% of hospitals (88% of beds) are privately owned. 30 of the 43 tertiary hospitals are run by private universities. 10 more are run by publicly owned universities. Payment is made on a fee-for-service basis. There is no direct government subsidy for hospitals. This encourages hospitals to expand and discourages community services.
The Korea International Medical Association has been formed to encourage medical tourism. The Korea Times reported in a series of articles that Korean hospitals have a discriminatory pricing policy, charging foreigners two to three times more than the full-fee for locals. The paper revealed that the price disparity in medical fees for foreign patients is extremely high, considering that the difference between the lowest and highest fees for the most-sought-after procedures exceeds more than 10 times on average. It claimed the government is overlooking soaring medical fees on foreign patients, who are unprotected from malpractice, discriminatory charging, overpricing and patient privacy rights under the Korean Medical Law.
Drinking alcohol
According to the World Health Organization, South Koreans rank No. 28 in alcohol consumption over all (2015) and No. 22 in the OECD (2013). According to Euromonitor data, it is number 1 in hard-liquor conspumption (2013). Age-standardized death rate of liver cirrhosis for male in South Korea is 20.6% of which 70.5% is attributed to alcohol. Prevalence of alcohol use disorders (including alcohol dependence and harmful use of alcohol) is 10.3% of male in South Korea, more than twice of 4.6% of Western Pacific Region.
Air pollution
According to the Environmental Performance Index 2016, South Korea ranked 173rd out of 180 countries in terms of air quality. More than 50 percent of the populations in South Korea exposed to dangerous levels of fine dust.
Chronic disease
According to the Ministry of Health and Welfare, chronic illness account for the majority of diseases in South Korea, a condition exacerbated by the health care system’s focus on treatment rather than prevention. The incidence of chronic disease in South Korea hovers around 24 percent. The human immunodeficiency virus (HIV) rate of prevalence at the end of 2003 was less than 0.1 percent. In 2001 central government expenditures on health care accounted for about 6 percent of gross domestic product (GDP). South Korea is experiencing a growing elderly population, which leads to an increase in chronic degenerative diseases. The proportion of the population over 65 is expected to rise from 13% in 2014 to 38% in 2050. Majority of health care professionals treat patients on curative, rather than preventive treatments, because of the lack of financial incentives for preventive treatments.
Unequal distribution of physicians
There are regional disparities between urban and rural areas for health professionals. The number of primary care doctors in cities is 37.3% higher than rural areas, and the problem is growing because younger physicians are choosing to practice in the cities.