
 | ||
Health care reform is a general rubric used for discussing major health policy creation or changes—for the most part, governmental policy that affects health care delivery in a given place. Health care reform typically attempts to:
Contents
- United States
- Hawaii and Massachusetts
- Health Care Costs
- United Kingdom
- Germany
- The Netherlands
- Russia
- Taiwan
- Elsewhere
- References
United States
In the United States, the debate regarding health care reform includes questions of a right to health care, access, fairness, sustainability, quality and amounts spent by government. The mixed public-private health care system in the United States is the most expensive in the world, with health care costing more per person than in any other nation, and a greater portion of gross domestic product (GDP) is spent on it than in any other United Nations member state except for East Timor (Timor-Leste). A study of international health care spending levels in the year 2000, published in the health policy journal Health Affairs, found that while the U.S. spends more on health care than other countries in the Organization for Economic Co-operation and Development (OECD), the use of health care services in the U.S. is below the OECD median by most measures. The authors of the study concluded that the prices paid for health care services are much higher in the U.S.
In spite of the amount spent on health care in the U.S., according to a 2008 Commonwealth Fund report, the United States ranks last in the quality of health care among developed countries. The World Health Organization (WHO), in 2000, ranked the US health care system 37th in overall performance and 72nd by overall level of health (among 191 member nations included in the study). International comparisons that could lead to conclusions about the quality of the health care received by Americans are subject to debate. The US pays twice as much yet lags other wealthy nations in such measures as infant mortality and life expectancy, which are among the most widely collected, hence easily compared, international statistics. Many people are underinsured, for example, in Colorado "of those with insurance for a full year, 36.3% were underinsured." About 10.7 million insured Americans spend more than a quarter of their annual paychecks on health care because of the high deductible polices.
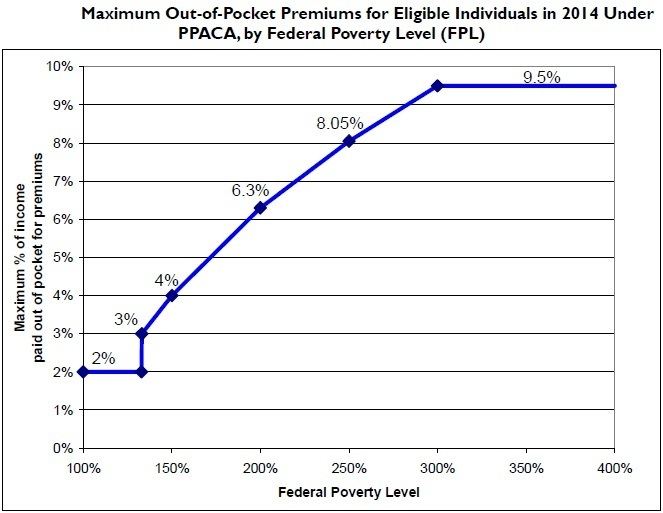
The Patient Protection and Affordable Care Act (Public Law 111-148) was signed into law by President Barack Obama on March 23, 2010. Along with the Health Care and Education Reconciliation Act of 2010 (signed March 30), the Act is a product of the health care reform efforts of the Democratic 111th Congress and the Obama administration. The law includes health-related provisions to take effect over the next four years, including expanding Medicaid eligibility for people making up to 133% of the federal poverty level (FPL), subsidizing insurance premiums for people making up to 400% of the FPL ($88,000 for family of 4 in 2010) so their maximum "out-of-pocket" payment for annual premiums will be from 2% to 9.5% of income, providing incentives for businesses to provide health care benefits, prohibiting denial of coverage and denial of claims based on pre-existing conditions, establishing health insurance exchanges, prohibiting insurers from establishing annual coverage caps, and support for medical research. According to White House and Congressional Budget Office figures, the maximum share of income that enrollees would have to pay for the "silver" healthcare plan would vary depending on their income relative to the federal poverty level, as follows: for families with income 133–150% of FPL will be 3-4% of income, for families with income of 150–200% of FPL will be 4-6.3% of income, for families with income 200–250% of FPL will be 6.3-8.05% of income, for families with income 250-300% of FPL will be 8.05-9.5% of income, for families with income from 300 to 400% of FPL will be 9.5% of income.
The costs of these provisions are offset by a variety of taxes, fees, and cost-saving measures, such as new Medicare taxes for those in high-income brackets, taxes on indoor tanning, cuts to the Medicare Advantage program in favor of traditional Medicare, and fees on medical devices and pharmaceutical companies; there is also a tax penalty for those who do not obtain health insurance, unless they are exempt due to low income or other reasons. The Congressional Budget Office estimates that the net effect of both laws will be a reduction in the federal deficit by $143 billion over the first decade.
The universal health care proposal pending in the U.S. Congress is called the United States National Health Care Act (H.R. 676, formerly the "Medicare for All Act.") The Congressional Budget Office and related government agencies scored the cost of a universal health care system several times since 1991, and have uniformly predicted cost savings, probably because of the 40% cost savings associated with universal preventative care and elimination of insurance company overhead costs.
In 2009, the Health Information Technology for Economic and Clinical Health Act (HITECH) offered monetary incentives from 2011 to 2015 for adopting EHR technology to decrease the length of time for hospitals and other healthcare facilities to move from paper records to an electronic health record system. The technology, while not without its pitfalls, should allow easier documentation and storage, the ability to access the information from a bedside, and the ability to sync prescriptions with a bar code.
The Affordable Care Act was enacted with the goals of increasing the quality and affordability of health insurance, lowering the uninsured rate by expanding public and private insurance coverage, and reducing the costs of healthcare for individuals and the government. Health care providers receive payment more frequently as the number of insured people increases and the number of uninsured patients unable to pay out of pocket declines. Competition between insurers in the new health insurance marketplace has increased pressure on insurance companies to reduce premium rates, leading to reduced compensation rates to providers in some plans.
Many healthcare facilities are struggling to break even since the cost of providing health services has increased, due to wages, technology, and resources. Medicare reimbursement payments to health providers for orthopaedic procedures such as total knee arthroplasty, lumbar spine repair, open rotator cuff repair, and open ankle fracture repair, declined from 1992-2010 which means the providers must rely on self-pay patients and patients with commercial insurances to make up the difference. The changes in regulations regarding risk pool assessment and the inclusion of 10 essential health benefits to every insurance plan have also contributed to the rise in cost of insurance premiums.
Hawaii and Massachusetts
Both Hawaii and Massachusetts have implemented some incremental reforms in health care, but neither state has complete coverage of its citizens. For example, data from the Kaiser Family Foundation shows that 5% of Massachusetts and 8% of Hawaii residents are uninsured. To date, The U.S. Uniform Law Commission, sponsored by the National Conference of Commissioners on Uniform State Laws has not submitted a uniform act or model legislation regarding health care insurance or health care reform.
Health Care Costs
The United States spends more on health care than any other country in the world, and, yet, has poorer health status by many measures. In 2007, the United States spent $7,290 per capita on health care. The average among peer nations in the Organisation for Economic Cooperation and Development (OECD) is $3075, just 42 percent of U.S. spending. Health spending is concentrated on a few consumers. In 2006, almost half of all health care spending was used to treat just 5 percent of the population, according to the Kaiser Family Foundation. More than half of bankruptcy filings are related to health care expenses, and sixty-eight percent of these cases are filed by people who have health insurance. According to the White House Council of Economic Advisors, the average family income will be $2,600 lower by 2020, if the growth in the cost of health care is not slowed by at least 1.5 percent. The cost of health insurance premiums more than doubled between 1999 and 2008 while workers' earnings stagnated. In 2008, the average annual cost for family insurance coverage was $12,700. 6
An estimated 52 million people - more than 15 percent of the people in the United States - are currently without health insurance or access to a government health care program. About 4 million people lost their health insurance during the current recession. That's more than 10,000 people every day. Nationally, 77 percent of the people who are uninsured are workers or are dependents of someone who works. In 2008, employees of small businesses contributed an average of $4,101 for family coverage, compared to $2,982 paid by employees in large firms. About 59 percent of employees with incomes below the poverty level ($18,310 for a family of three)11 do not have health insurance. At income levels twice to three times the poverty level, about 34 percent lack insurance. Half as many lack insurance at four times the poverty level.
United Kingdom
Healthcare was reformed in 1948 after the Second World War, broadly along the lines of the 1942 Beveridge Report, with the creation of the National Health Service or NHS. It was originally established as part of a wider reform of social services and funded by a system of National Insurance, though receipt of healthcare was never contingent upon making contributions towards the National Insurance Fund. Private health care was not abolished but had to compete with the NHS. About 15% of all spending on health in the UK is still privately funded but this includes the patient contributions towards NHS provided prescription drugs, so private sector healthcare in the UK is quite small. As part of a wider reform of social provision it was originally thought that the focus would be as much about the prevention of ill-health as it was about curing disease. The NHS for example would distribute baby formula milk fortified with vitamins and minerals in an effort to improve the health of children born in the post war years as well as other supplements such as cod liver oil and malt. Many of the common childhood diseases such as measles, mumps, and chicken pox were mostly eradicated with a national program of vaccinations.
The NHS has been through many reforms since 1974. The Conservative Thatcher administrations attempted to bring competition into the NHS by developing a supplier/buyer role between hospitals as suppliers and health authorities as buyers. This necessitated the detailed costing of activities, something which the NHS had never had to do in such detail, and some felt was unnecessary. The Labour Party generally opposed these changes, although after the party became New Labour, the Blair government retained elements of competition and even extended it, allowing private health care providers to bid for NHS work. Some treatment and diagnostic centres are now run by private enterprise and funded under contract. However, the extent of this privatisation of NHS work is still small, though remains controversial. The administration committed more money to the NHS raising it to almost the same level of funding as the European average and as a result, there was large expansion and modernisation programme and waiting times improved.
The government of Gordon Brown proposed new reforms for care in England. One is to take the NHS back more towards health prevention by tackling issues that are known to cause long term ill health. The biggest of these is obesity and related diseases such as diabetes and cardio-vascular disease. The second reform is to make the NHS a more personal service, and it is negotiating with doctors to provide more services at times more convenient to the patient, such as in the evenings and at weekends. This personal service idea would introduce regular health check-ups so that the population is screened more regularly. Doctors will give more advice on ill-health prevention (for example encouraging and assisting patients to control their weight, diet, exercise more, cease smoking etc.) and so tackle problems before they become more serious. Waiting times, which fell considerably under Blair (median wait time is about 6 weeks for elective non-urgent surgery) are also in focus. A target was set from December 2008, to ensure that no person waits longer than 18 weeks from the date that a patient is referred to the hospital to the time of the operation or treatment. This 18 week period thus includes the time to arrange a first appointment, the time for any investigations or tests to determine the cause of the problem and how it should be treated. An NHS Constitution was published which lays out the legal rights of patients as well as promises (not legally enforceable) the NHS strives to keep in England.
Germany
Numerous healthcare reforms in Germany were legislative interventions to stabilise the public health insurance since 1983. 9 out of 10 citizens are publicly insured, only 8% privately. Health care in Germany, including its industry and all services, is one of the largest sectors of the German economy. The total expenditure in health economics of Germany was about 287.3 billion euro in 2010, equivalent to 11.6 percent of the gross domestic product (GDP) this year and about 3,510 euro per capita. Direct inpatient and outpatient care equal just about a quarter of the entire expenditure - depending on the perspective. Expenditure on pharmaceutical drugs is almost twice the amount of those for the entire hospital sector. Pharmaceutical drug expenditure grew by an annual average of 4.1% between 2004 and 2010.
These developments have caused numerous healthcare reforms since the 1980s. An actual example of 2010 and 2011: First time since 2004 the drug expenditure fell from 30.2 billion euro in 2010, to 29.1 billion Euro in 2011, i. e. minus 1.1 billion Euro or minus 3.6%. That was caused by restructuring the Social Security Code: manufacturer discount 16% instead of 6%, price moratorium, increasing discount contracts, increasing discount by wholesale trade and pharmacies.
The Netherlands
The Netherlands has introduced a new system of health care insurance based on risk equalization through a risk equalization pool. In this way, a compulsory insurance package is available to all citizens at affordable cost without the need for the insured to be assessed for risk by the insurance company. Furthermore, health insurers are now willing to take on high risk individuals because they receive compensation for the higher risks.
A 2008 article in the journal Health Affairs suggested that the Dutch health system, which combines mandatory universal coverage with competing private health plans, could serve as a model for reform in the US.
Russia
Following the collapse of the Soviet Union, Russia embarked on a series of reforms intending to deliver better healthcare by compulsory medical insurance with privately owned providers in addition to the state run institutions. According to the OECD none of 1991-93 reforms worked out as planned and the reforms had in many respects made the system worse. Russia has more physicians, hospitals, and healthcare workers than almost any other country in the world on a per capita basis, but since the collapse of the Soviet Union, the health of the Russian population has declined considerably as a result of social, economic, and lifestyle changes. However, after Putin became president in 2000 there was significant growth in spending for public healthcare and in 2006 it exceed the pre-1991 level in real terms. Also life expectancy increased from 1991-93 levels, infant mortality rate dropped from 18.1 in 1995 to 8.4 in 2008. Russian Prime Minister Vladimir Putin announced a large-scale health care reform in 2011 and pledged to allocate more than 300 billion rubles ($10 billion) in the next few years to improve health care in the country.
Taiwan
Taiwan changed its healthcare system in 1995 to a National Health Insurance model similar to the US Medicare system for seniors. As a result, the 40% of Taiwanese people who had previously been uninsured are now covered. It is said to deliver universal coverage with free choice of doctors and hospitals and no waiting lists. Polls in 2005 are reported to have shown that 72.5% of Taiwanese are happy with the system, and when they are unhappy, it's with the cost of premiums (equivalent to less than US$20 a month).
Employers and the self-employed are legally bound to pay National Health Insurance (NHI) premiums which are similar to social security contributions in other countries. However, the NHI is a pay-as-you-go system. The aim is for the premium income to pay costs. The system is also subsidized by a tobacco tax surcharge and contributions from the national lottery.
Elsewhere
As evidenced by the large variety of different healthcare systems seen across the world, there are several different pathways that a country could take when thinking about reform. In comparison to the UK, physicians in Germany have more bargaining power through professional organizations (i.e., physician associations); this ability to negotiate affects reform efforts. Germany makes use of sickness funds, which citizens are obliged to join but are able to opt out if they have a very high income (Belien 87). The Netherlands used a similar system but the financial threshold for opting out was lower (Belien 89). The Swiss, on the other hand use more of a privately based health insurance system where citizens are risk-rated by age and sex, among other factors (Belien 90). The United States government provides healthcare to just over 25% of its citizens through various agencies, but otherwise does not employ a system. Healthcare is generally centered around regulated private insurance methods.
One key component to healthcare reform is the reduction of healthcare fraud and abuse. In the U.S. and the EU, it is estimated that as much as 10 percent of all healthcare transactions and expenditures may be fraudulent. See Terry L. Leap, Phantom Billing, Fake Prescriptions, and the High Cost of Medicine: Health Care Fraud and What to do about It (Cornell University Press, 2011).
Also interesting to notice is the oldest healthcare system in the world and its advantages and disadvantages, see Health in Germany.