
ICD-9-CM 315.31 | ICD-10 F80.1 MeSH D001039 | |
 | ||
Expressive aphasia (non-fluent aphasia) is characterized by the loss of the ability to produce language (spoken or written). A person with expressive aphasia will exhibit effortful speech. Speech may only include important content words and leave out insignificant words, like "the". This is known as "telegraphic speech". The person may still be understood, but sentences will not be grammatical. In very severe forms of Expressive Aphasia, a person may only speak using single word utterances. It is one subset of a larger family of disorders known collectively as aphasia. Expressive aphasia differs from dysarthria, which is typified by a patient's inability to properly move the muscles of the tongue and mouth to produce speech. Expressive aphasia also differs from apraxia of speech which is a motor disorder characterized by an inability to create and sequence motor plans for speech. Comprehension is typically only mildly to moderately impaired in expressive aphasia due to difficulty understanding complex grammar. This contrasts with receptive aphasia, which is distinguished by a patient's inability to comprehend language or speak with appropriately meaningful words. Expressive aphasia is also known as Broca's aphasia in clinical neuropsychology and agrammatic aphasia in cognitive neuropsychology and is caused by acquired damage to the anterior regions of the brain, such as the left posterior inferior frontal gyrus or inferior frontal operculum, also described as Broca's area (Brodmann area 44 and Brodmann area 45). Expressive aphasia is also a symptom of some migraine attacks.
Contents
- Signs and symptoms
- Overlap with receptive aphasia
- Causes
- Diagnosis
- Treatment
- Singing and Melodic Intonation Therapy
- Constraint induced therapy
- Pharmacotherapy
- Transcranial magnetic stimulation
- Treatment of underlying forms
- Mechanisms of recovery
- Speech entrainment a potential new treatment
- Prognosis
- History
- Society and culture
- Notable cases
- References
Signs and symptoms
Broca's aphasia is a type of expressive aphasia because speech production is halting and effortful. Damage is typically in the anterior portion of the left hemisphere. Typically, writing is at least as severely impaired as speech. Persons with Broca's aphasia are usually aware of their communication deficits, and are more prone to depression and sometimes catastrophic reactions than are patients with other forms of aphasia. Intonation and stress patterns are deficient. Language is reduced to disjointed words, and sentence construction is poor, omitting function words and inflections (bound morphemes). A person with expressive aphasia might say "Son ... University ... Smart ... Good ... Good ... "Content words (nouns, verbs) may be used in speech, but sentences are difficult to produce due to problems with grammar, resulting in "telegraphic speech." In its more severe form, spoken utterances may be reduced to single words. "The prosody of those with Broca's aphasia is compromised by shortened length of utterances and the presence of self-repairs and disfluencies."
For example, in the following passage, a Broca's aphasic patient is trying to explain how he came to the hospital for dental surgery:
Yes... ah... Monday... er... Dad and Peter H... (his own name), and Dad.... er... hospital... and ah... Wednesday... Wednesday, nine o'clock... and oh... Thursday... ten o'clock, ah doctors... two... an' doctors... and er... teeth... yah.Patients who communicated with sign language before the onset of the aphasia experience analogous symptoms.
Severity of expressive aphasia varies among patients. In the most extreme cases, patients may be able to produce only a single word. The most famous case of this was Paul Broca's patient Leborgne, nicknamed "Tan", after the only syllable he could say. Even in such cases, over-learned and rote-learned speech patterns may be retained—for instance, some patients can count from one to ten, but cannot produce the same numbers in ordinary conversation.
Meanwhile, in general, word comprehension is preserved; making most Broca's aphasia patients receptive language functional. Individuals with Broca's aphasia understand most of the everyday conversation around them, but higher-level deficits in receptive language can also occur. Individuals with Broca's aphasia can often respond to simple questions. For more complex sentences, with many steps interpretation dependent on syntax and phrase structure is substantially impaired. This can be demonstrated by using phrases with unusual structures. A typical Broca's aphasic patient will misinterpret "the man is bitten by the dog" by switching the subject and object. Note this element is a problem with receptive language, not expressive language, and is one reason why the problem is referred to as agrammatic aphasia. Because patients with Broca's aphasia have good receptive language, their reading skills are also functional.
Patients who recover go on to say that they knew what they wanted to say but could not express themselves. Residual deficits will often be seen.
Agrammatic aphasiacs tend to be sensitive to word order, relying instead on pragmatics in order to understand others. For example, they may understand a sentence such as “The teenagers arrested the cop” to actually mean “The cop arrested the teenagers”. This is due to the understood meaning to be more realistic and more likely to happen. Because of this trouble with understanding, there is a mental leap that is often made in order to attempt comprehension. It is possible that people with agrammatic aphasia rely on a heuristic based on the canonical word order of English. Typically, the noun phrase preceding the verb takes on the role of the agent, or the noun that does the verb. Additionally, the noun phrase following a preposition such as ‘by’ is also assigned the role of agent, and thus follows the same thought process. Relying on this heuristic helps to understand reversible active sentences.
For example, only 75% of agrammatic aphasiacs would comprehend the reversible active sentence, “The actor applauded the dancer” accurately, due to the atypical scenario that the sentence describes. Reversible passive sentences such as “The actor was applauded by the dancer” are even more complex and difficult to comprehend, and were only found to be accurately understood by 50% of tested agrammatic aphasiacs in one study. Some researchers hypothesize that Broca’s aphasiacs struggle with such types of sentence processing due to damage to a specific sentence processing mechanism that connects an antecedent with its trace. Broca’s aphasicas also have been found to struggle in the integration of syntactic structure of a sentence with semantic information. This can perhaps be attributed to the a timing problem where lexical items are retrieved too slowly to integrate with sentence structure.
Overlap with receptive aphasia
In addition to difficulty expressing oneself, sufferers of expressive aphasia are also noted to commonly have trouble with comprehension in certain linguistic areas. This agrammatism overlaps with receptive aphasia, but can be seen in patients of expressive aphasia without being diagnosed as having receptive aphasia too. The most well-noted of these are object-relative clauses, object Wh- questions, and topicalized structures (placing the topic at the beginning of the sentence). These three concepts all share phrasal movement, which can cause words to lose their thematic roles when they change order in the sentence. This is often not an issue for people without agrammatic aphasias, but many aphasics rely very heavily on word order to understand roles that words play within the sentence.
Causes
The most common cause of expressive aphasia is stroke. A stroke is caused by hypoperfusion (lack of oxygen) to an area of the brain, which is commonly caused by thrombosis or embolism. Some form of aphasia occurs in 34 to 38% of stroke patients. Expressive aphasia occurs in approximately 12% of new cases of aphasia caused by stroke. In most cases, expressive aphasia is caused by a stroke in Broca's area or the surrounding vicinity. However, cases of expressive aphasia have been seen in patients with strokes in other areas of the brain. Patients with classic symptoms of expressive aphasia in general have more acute brain lesions, whereas patients with larger, widespread lesions exhibit a variety of symptoms that may be classified as global aphasia or left unclassified.
Expressive aphasia can also be caused by trauma to the brain, tumor, cerebral hemorrhage by extradural hematoma.
Understanding lateralization of brain function is important for understanding what areas of the brain cause expressive aphasia when damaged. In the past, it has been believed that the area for language production differs between left and right-handed individuals. If this were true, damage to the homologous region of Broca's area in the right hemisphere should cause aphasia in a left-handed individual. More recent studies have shown that even left-handed individuals typically have language functions only in the left hemisphere. However, left-handed individuals are more likely to have a dominance of language in the right hemisphere.
Diagnosis
Expressive aphasia is also a classification of non-fluent aphasia, as opposed to fluent aphasia. Diagnosis is done on a case by case basis, as lesions often affect surrounding cortex and deficits are not well conserved between patients.
In order to diagnose a patient who is suffering from Broca’s aphasia, there are certain commonly used tests and procedures. The Boston Diagnostic Aphasia Examination (BDAE), the Western Aphasia Battery (WAB) and the Porch Index of Speech Ability (PISA) are all evaluations created for the purpose of identifying aphasia and the class of the condition the patient is experiencing. More routine processes for diagnosis include MRI scans and questions. The ability to name common objects, maintain casual conversation, proper word use, answering questions concerning a subject the patient read or heard, word and sentence repetition skills and general reading and writing proficiency are all determiners of possible expressive aphasia. Testing swallowing can also aid in diagnosing this impairment, as can the ability to use alternative and augmentative (AAC) speech, which is a form of communication specifically used by those suffering from physical or mental disabilities that impair the production of spoken or written language.
Treatment
Currently, there is no standard treatment for expressive aphasia. Most aphasia treatment is individualized based on a patient's condition and needs as assessed by a speech language pathologist. The majority of patients go through a period of spontaneous recovery following brain injury in which they regain a great deal of language function. In the months following injury or stroke, most patients receive traditional treatment for a few hours per day. Among other exercises, patients practice the repetition of words and phrases. Mechanisms are also taught in traditional treatment to compensate for lost language function such as drawing and using phrases that are easier to pronounce. Emphasis is placed on establishing a basis for communication with family and caregivers in everyday life. The following treatments are currently being studied to determine the best possible method for treating aphasia.
Treatment is also individualized based on the patient's own goals, along with the family's input. Also, treatment is in the language that the patient speaks in. Usually a bilingual Speech Language Pathologist or a trained interpreter will treat bilingual patients with Aphasia.
As a client, you may have the option of individual or group treatment. Group treatment tends to go under the radar but has been seen to have advantageous outcomes. Some types of group treatments include becoming a part of a supportive peer environment, family counseling, maintenance groups, support groups and treatment groups. These are important to consider because depression can be very common with Aphasia. It is important to keep your mental and emotional health strong, and by allowing yourself all of this support, we can ensure this.
Singing and Melodic Intonation Therapy
Melodic Intonation Therapy was inspired by the observation that individuals with non-fluent aphasia sometimes can sing words or phrases that they normally cannot speak."Melodic Intonation Therapy was begun as an attempt to use the intact melodic/prosodic processing skills of the right hemisphere in those with aphasia to help cue retrieval words and expressive language." It is believed that this is because singing capabilities are stored in the right hemisphere of the brain, which is likely to remain unaffected after a stroke in the left hemisphere. However, recent evidence demonstrates that the capability of individuals with aphasia to sing entire pieces of text may actually result from rhythmic features and the familiarity with the lyrics.
The goal of Melodic Intonation Therapy is to utilize singing to access the language-capable regions in the right hemisphere and use these regions to compensate for lost function in the left hemisphere. Because it was assumed that patients are better at singing phrases than speaking them, the natural musical component of speech was used to engage the patients' ability to voice phrases. Contrary to this assumption, a clinical study revealed that singing and rhythmic speech may be similarly effective in the treatment of non-fluent aphasia and apraxia of speech. Moreover, evidence from randomized controlled trials is still needed to confirm that Melodic Intonation Therapy is suitable to improve propositional utterances and speech intelligibility in individuals with (chronic) non-fluent aphasia and apraxia of speech.
Melodic Intonation Therapy appears to work particularly well in patients who have had a unilateral, left hemisphere stroke, show poor articulation, nonfluent or severely restricted speech output, can produce some intelligible words while singing, moderately well preserved auditory comprehension, good motivation and emotional stability. MIT therapy on average lasts for 1.5 hours per day for five days per week. At the lowest level of therapy, simple words and phrases (such as "water" and "I love you") are broken down into a series of high- and low-pitch syllables. With increased treatment, longer phrases are taught and less support is provided by the therapist. Patients are taught to say phrases using the natural melodic component of speaking and continuous voicing is emphasized. The patient is also instructed to use the left hand to tap the syllables of the phrase while the phrases are spoken. Tapping is assumed to trigger the rhythmic component of speaking to utilize the right hemisphere.
The efficacy of singing has been proven in one patient with aphasia who was a trained musician; in this patient, singing had an advantage over rhythmic speech. However, the advantage of singing over rhythmic speech was not observed in 10 patients without any musical background. FMRI studies have shown that Melodic Intonation Therapy uses both sides of the brain to recover lost function, as opposed to traditional therapies that utilize only the left hemisphere. Furthermore, it has been seen that, in MIT, individuals with small lesions in the left hemisphere seem to recover by activation of the left hemisphere perilesional cortex, while, in individuals with larger left-hemisphere lesions, there is a recruitment of the use of language-capable regions in the right hemisphere. The interpretation of these results is still a matter of debate. For example, it remains unclear whether changes in neural activity in the right hemisphere result from singing or from the intensive use of common phrases, such as "thank you," "how are you?" or "I am fine." This type of phrases falls into the category of formulaic language and is known to be supported by neural networks of the intact right hemisphere.
A pilot study reported positive results when comparing the efficacy of a modified form of MIT to no treatment in people with nonfluent aphasia with damage to their left-brain. A randomized controlled trial was conducted. The study reported benefits of utilizing modified MIT treatment early in the recovery phase for people with nonfluent aphasia.
Melodic Intonation Therapy is used by music therapists, board-certified professionals that use music as a therapeutic tool to effect certain non-musical outcomes in their patients. Speech language pathologists can also use this therapy for individuals who have had a left hemisphere stroke and non-fluent aphasias such as Broca’s or even apraxia of speech. Candidates will have good auditory comprehension, poor repetition and articulation skills, and good emotional stability and memory.
Constraint-induced therapy
Constraint-induced aphasia therapy (CIAT) is based on similar principles as constraint-induced movement therapy developed by Dr. Edward Taub at the University of Alabama at Birmingham. Constraint-induced movement therapy is based on the idea that a person with an impairment (physical or communicative) develops a "learned nonuse" by compensating for the lost function with other means such as using an unaffected limb by a paralyzed individual or drawing by a patient with aphasia. In constraint-induced movement therapy, the alternative limb is constrained with a glove or sling and the patient is forced to use the affected limb. In constraint-induced aphasia therapy, the interaction is guided by communicative need in a language game context, picture cards, barriers making it impossible to see other players' cards, and other materials, so that patients are encouraged ("constrained") to use the remaining verbal abilities to succeed in the communication game.
Two important principles of constraint-induced aphasia therapy are that treatment is very intense, with sessions lasting for up to 6 hours over the course of 10 days and that language is used in a communication context in which it is closely linked to (nonverbal) actions. These principles are motivated by neuroscience insights about learning at the level of nerve cells (synaptic plasticity) and the coupling between cortical systems for language and action in the human brain. Constraint-induced therapy contrasts sharply with traditional therapy by the strong belief that mechanisms to compensate for lost language function should not be used unless absolutely necessary, even in everyday life.
It is believed that CIAT works by the mechanism of increased neuroplasticity. By constraining an individual to use only speech, it is believed that the brain can reestablish old neural pathways and recruit new neural pathways to compensate for lost function.
The greatest advantage of CIAT has been seen in its treatment of chronic aphasia (lasting over 1 year). Studies of CIAT have shown that further improvement is possible even after a patient has reached a "plateau" period of recovery. It has also been proven that the benefits of CIAT are retained long term. However, improvements only seem to be made while a patient is undergoing intense therapy. A recent breakthrough has been achieved by combining constraint-induced aphasia therapy with drug treatment, which led to an amplification of therapy benefits.
Pharmacotherapy
In addition to active speech therapy, pharmaceuticals have also been considered as a useful treatment for expressive aphasia. This area of study is relatively new and much research continues to be conducted.
The following drugs have been suggested for use in treating aphasia and their efficacy has been studied in control studies.
The most effect has been shown by piracetam and amphetamine, which may increase cerebral plasticity and result in an increased capability to improve language function. It has been seen that piracetam is most effective when treatment is begun immediately following stroke. When used in chronic cases it has been much less efficient.
Bromocriptine has been shown by some studies to increase verbal fluency and word retrieval with therapy than with just therapy alone. Furthermore, its use seems to be restricted to non-fluent aphasia.
Donepezil has shown a potential for helping chronic aphasia.
No study has established irrefutable evidence that any drug is an effective treatment for aphasia therapy. Furthermore, no study has shown any drug to be specific for language recovery. Comparison between the recovery of language function and other motor function using any drug has shown that improvement is due to a global increase plasticity of neural networks. Pharmaceutical therapy remains an important area of study in aphasia treatment.
Transcranial magnetic stimulation
In transcranial magnetic stimulation (TMS), magnetic fields are used to create electrical currents in specified cortical regions. The procedure is a painless and noninvasive method of stimulating the cortex. TMS works by suppressing the inhibition process in certain areas of the brain. By suppressing the inhibition of neurons by external factors, the targeted area of the brain may be reactivated and thereby recruited to compensate for lost function. Research has shown that patients can show increased object naming ability with regular transcranial magnetic stimulation than patients in therapy without TMS. Furthermore, this improvement has been proven to be permanent and remains upon the completion of TMS therapy. However, some patients fail to show any significant improvement from TMS which indicates the need for further research of this treatment.
Treatment of underlying forms
Described as the linguistic approach to the treatment of expressive aphasia, treatment begins by emphasizing and educating patients on the thematic roles of words within sentences. Sentences that are usually problematic will be reworded into active-voiced, declarative phrasings of their non-canonical counterparts. The simpler sentence phrasings are then transformed into variations that are more difficult to interpret. For example, many sufferers of expressive aphasia struggle with Wh- sentences. "What" and "who" questions are problematic sentences that this treatment method attempts to improve, and they are also two interrogative particles that are strongly related to each other because they reorder arguments from the declarative counterparts. For instance, therapists have used sentences like, "Who is the boy helping?" and "What is the boy fixing?" because both verbs are transitive- they require two arguments in the form of a subject and a direct object, but not necessarily an indirect object. In addition, certain question particles are linked together based on how the reworded sentence is formed. Training "who" sentences increased the generalizations of non-trained "who" sentences as well as untrained "what" sentences, and vice versa. Likewise, "where" and "when" question types are very closely linked. "What" and "who" questions alter placement of arguments, and "where" and "when" sentences move adjunct phrases. Training is in the style of: "The man parked the car in the driveway. What did the man park in the driveway?" Sentence training goes on in this manner for more domains, such as clefts and sentence voice.
Results: Patients’ use of sentence types used in the TUF treatment will improve, subjects will generalize sentences of similar category to those used for treatment in TUF, and results are applied to real-world conversations with others. Generalization of sentence types used can be improved when the treatment progresses in the order of more complex sentences to more elementary sentences. Treatment has been shown to affect on-line (real-time) processing of trained sentences and these results can be tracked using fMRI mappings. Training of Wh- sentences has led improvements in three main areas of discourse for aphasics: increased average length of utterances, higher proportions of grammatical sentences, and larger ratios of numbers of verbs to nouns produced. Patients also showed improvements in verb argument structure productions and assigned thematic roles to words in utterances with more accuracy. In terms of on-line sentence processing, patients having undergone this treatment discriminate between anomalous and non-anomalous sentences with more accuracy than control groups and are closer to levels of normalcy than patients not having participated in this treatment.
Mechanisms of recovery
Mechanisms for recovery differ from patient to patient. Some mechanisms for recovery occur spontaneously after damage to the brain, whereas others are caused by the effects of language therapy. FMRI studies have shown that recovery can be partially attributed to the activation of tissue around the damaged area and the recruitment of new neurons in these areas to compensate for the lost function. Recovery may also be caused in very acute lesions by a return of blood flow and function to damaged tissue that has not died around an injured area. It has been stated by some researchers that the recruitment and recovery of neurons in the left hemisphere opposed to the recruitment of similar neurons in the right hemisphere is superior for long-term recovery and continued rehabilitation. It is thought that, because the right hemisphere is not intended for full language function, using the right hemisphere as a mechanism of recovery is effectively a "dead-end" and can lead only to partial recovery.
It has been proven that, among all types of therapies, one of the most important factors and best predictors for a successful outcome is the intensity of the therapy. By comparing the length and intensity of various methods of therapies, it was proven that intensity is a better predictor of recovery than the method of therapy used.
Speech entrainment: a potential new treatment
In a 2012 study from the University of South Carolina's Arnold School of Public Health, researchers found that some stroke victims with speech loss from Broca's aphasia can speak fluently through the use of "speech entrainment". In the experiment of 13 people with Broca's aphasia, each subject was prompted with an auditory and visual stimulus of a series of sentences. The visual stimulus was a video shown on an iPod of someone speaking each sentence in time with an audio recording of each sentence. The result of this audio-visual stimulation was amazing: the patients, some who had Broca's aphasia for multiple decades, were able to mimic the movements of the mouth in real time and speak fluently. Though there are various methods of treatment for Broca's aphasia as stated on this page, speech entrainment provides a potential future therapeutic method that produces drastic results simply not seen in any other method of treatment.
Prognosis
In most individuals with expressive aphasia, the majority of recovery is seen within the first year following a stroke or injury. The majority of this improvement is seen in the first four weeks in therapy following a stroke and slows thereafter. However, this timeline will vary depending upon the type of stroke experienced by the patient. Patients who experienced an ischemic stroke may recover in the days and weeks following the stroke, and then experience a plateau and gradual slowing of recovery. On the other hand, patients who experienced a hemorrhagic stroke experience a slower recovery in the first 4–8 weeks, followed by a faster recovery which eventually stabilizes.
When compared to patients with the most common types of aphasia, patients with expressive aphasia tend to show the most improvement within the first year. This may be due to an expressive aphasiac's awareness and greater insight of their impairment (unlike in receptive aphasia), which motivates him/her to progress in treatment. Studies have also found that prognosis of expressive aphasia correlates strongly with the initial severity of impairment. Those with the greatest initial disability tend to show the greatest improvement among test groups. Within the first year, the diagnosis of patients with expressive aphasia may change to anomic aphasia. Likewise, patients diagnosed with global aphasia may be re-diagnosed with expressive aphasia upon improvement. Typically, little improvement is seen after the first year following a stroke. However, it has been seen that continued recovery is possible years after a stroke with effective treatment using methods such as constraint-induced aphasia therapy. Depression, anxiety, and social withdrawal are all factors which have been proven to negatively affect a person's chance of recovery. Due to frustration from the inability to express themselves, sufferers of expressive aphasia can become clinically depressed. This creates further impairment because the left hemisphere in depressed individuals functions at lower levels of activity than people without depression. This further complicates issues because the decreased functionality of the two conditions can combine to create even lower levels of activity than in either of the two conditions alone. The strategy for aiding individuals in this condition is to deal with the depression first. Once the depression is alleviated, or at least under control, the patient is better able to focus on treatments that target the aphasia than if the order of treatments was reversed.
Location and size of the brain lesion may also play a role in the prognosis of aphasia. It has been seen in receptive aphasia that larger lesions correlate to slower recovery. It has also been seen that patients with aphasia caused by sub cortical lesions have a better chance of recovery than those with aphasia due to cortical stroke. Other factors that may affect recovery are age, education, social support, and handedness (how one's brain is organized).
History
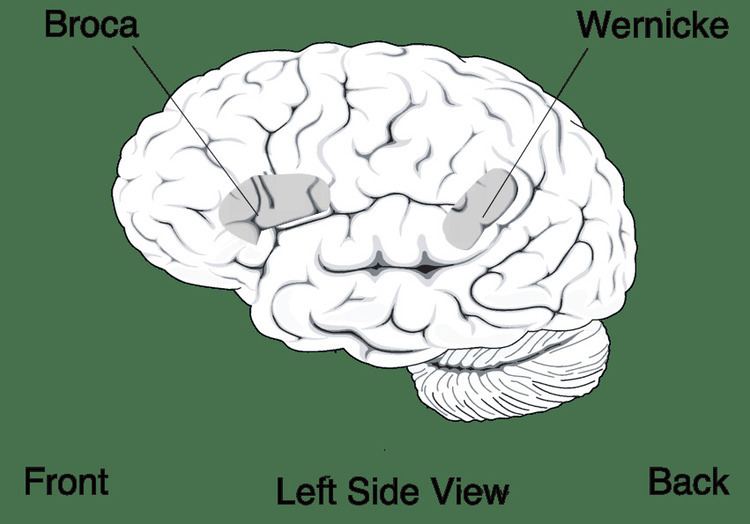
Expressive aphasia was first identified by the French neurologist Paul Broca. By examining the brains of deceased individuals having acquired expressive aphasia in life, he concluded that language ability is localized in the ventroposterior region of the frontal lobe. One of the most important aspects of Paul Broca's discovery was the observation that the loss of proper speech in expressive aphasia is due to the brain's loss of ability to produce language, as opposed to the mouth's loss of ability to produce words.
The discoveries of Paul Broca were made during the same period of time as the German Neurologist Carl Wernicke, who was also studying brains of aphasiacs post-mortem and identified the region now known as Wernicke's area. Discoveries of both men contributed to the concept of localization, which states that specific brain functions are all localized to a specific area of the brain. While both men made significant contributions to the field of aphasia, it was Carl Wernicke who realized the difference between patients with aphasia that could not produce language and those that could not comprehend language (the essential difference between expressive and receptive aphasia).
Society and culture
The protagonist of Stephen King's novel Duma Key exhibited symptoms of a condition similar to receptive aphasia after suffering brain damage in an industrial accident. When trying to recall some words, he would frequently substitute a synonym of a similar-sounding word, such as trying to say "char" but instead saying "burn" (a synonym of "char") and "friend" (a synonym of "chum").
The character Toggle in Garry Trudeau's cartoon strip Doonesbury suffers from expressive aphasia.
The character Saxifrage Russell suffers Broca's aphasia due to a stroke suffered while being rescued from interrogators in Kim Stanley Robinson's novel Green Mars.
The character Hodor in George R. R. Martin's A Song of Ice and Fire may have suffered a form of Broca's aphasia. Throughout the novels, Hodor is only able to say the single word "Hodor." The characters of the novels associate the word with him and use it as his name despite it not being the name that he was born with. "Martin doesn't provide any details regarding whether Hodor suffered a traumatic brain injury as a child. But his symptoms are consistent with this type of disorder." The character in the TV series also carries a scar on his temple which would be the correct location for a lesion in Broca's area.
Similar to the above, the character Emmeryn in Nintendo's Fire Emblem: Awakening shows signs of this condition after a presumably traumatic injury, along with what seems to be amnesia.