
ICD-10 E80.0 (ILDS E80.010) OMIM 177000 eMedicine derm/473 | ICD-9-CM 277.1 DiseasesDB 4484 | |
 | ||
Specialty endocrinology, dermatology | ||
Erythropoietic protoporphyria (EPP) is a form of porphyria, which varies in severity and can be very painful. It arises from a deficiency in the enzyme ferrochelatase, leading to abnormally high levels of protoporphyrin in the erythrocytes, plasma, skin and liver. The severity varies significantly from individual to individual.
Contents
- Presentation
- Liver failure in EPP
- EPP and pregnancy
- Genetics
- Pathophysiology
- Diagnosis
- Treatment and prognosis
- Approved therapies
- Off label use
- Epidemiology
- History
- Popular culture
- References
A clinically similar form of porphyria, known as X-Linked dominant protoporphyria, was identified in 2008.
Presentation
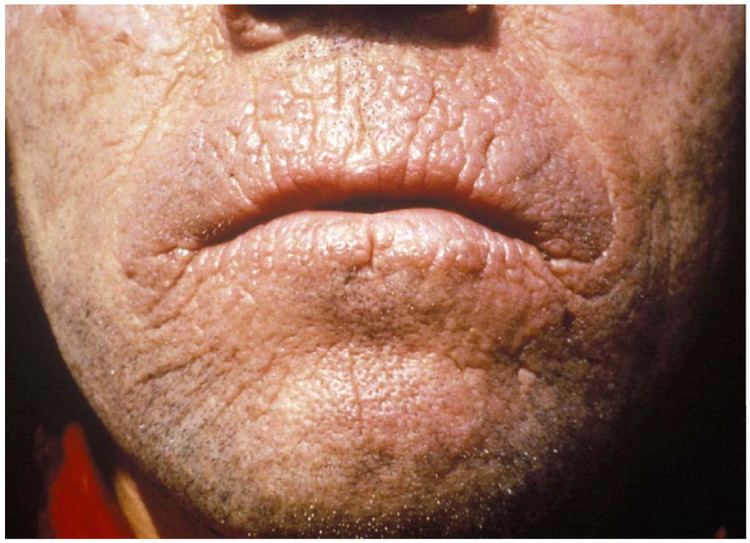
EPP usually presents in childhood with the commonest mode of presentation as acute photosensitivity of the skin. It affects areas exposed to the sun and tends to be intractable. A few minutes of exposure to the sun induces pruritus, erythema, swelling and pain. Longer periods of exposure may induce second degree burns. After repetitive exposure, patients may present with lichenification, hypopigmentation, hyperpigmentation and scarring of the skin.
EPP usually first presents in childhood, and most often affects the face and the upper surfaces of the arms, hands, and feet and the exposed surfaces of the legs. Most patients, if the EPP is not as severe, manifest symptoms with onset of puberty when the male and female hormone levels elevate during sexual development and maintenance. More severe EPP can manifest in infancy. EPP can be triggered through exposure to sun even though the patient is behind glass. Even the UV emissions from arc welding with the use of full protective mask have been known to trigger EPP. EPP can also manifest between the ages of 3 and 6.
Prolonged exposure to the sun can lead to edema of the hands, face, and feet, rarely with blistering and petechiae. Skin thickening can sometimes occur over time.
People with EPP are also at increased risk to develop gallstones. One study has noted that EPP patients suffer from vitamin D deficiency.
Liver failure in EPP
Protoporphyrin accumulates to toxic levels in the liver in 5-20% of EPP patients, leading to liver failure. The spectrum of hepatobiliary disease associated with EPP is wide. It includes cholelithiasis, mild parenchymal liver disease, progressive hepatocellular disease and end-stage liver disease.
A lack of diagnostic markers for liver failure makes it difficult to predict which patients may experience liver failure, and the mechanism of liver failure is poorly understood. A retrospective European study identified 31 EPP patients receiving a liver transplant between 1983 and 2008, with phototoxic reactions in 25% of patients who were unprotected by surgical light filters. The same study noted a 69% recurrence of the disease in the grafted organ. Five UK liver transplants for EPP have been identified between 1987 and 2009.
Frequent liver testing is recommended in EPP patients where no effective therapy has been identified to manage liver failure to date.
EPP and pregnancy
EPP photosensitivity symptoms are reported to lessen in some female patients during pregnancy and menstruation, although this phenomenon is not consistent, and the mechanism is not understood.
Genetics
Most cases of EPP are results of inborn errors of metabolism but the metabolic defect in some patients may be acquired. Mutation of the gene that encodes for ferrochelatase in the long arm of chromosome 18 is found in majority of the cases. Ferrochelatase (FECH) catalyzes the insertion of ferrous iron into the protoporphyrin IX ring to form heme. EPP exhibits both recessive and dominant patterns of inheritance and a high degree of allelic heterogeneity with incomplete penetrance. Most heterozygotes are asymptomatic. Symptoms do not occur unless FECH activity is less than 30% of normal, but such low levels are not present in a majority of patients.
Pathophysiology
Cells which synthesize heme are predominantly erythroblasts/reticulocytes in the bone marrow (80%) and hepatocytes (20%). Deficiency of FECH results in increased release of protoporphyrin, which binds to albumin in plasma and subsequently undergoes hepatic extraction. Normally, most protoporphyrin in hepatocytes is secreted into bile; the remainder undergoes transformation into heme. Some protoporphyrin in bile is returned to the liver as a consequence of the enterohepatic circulation; the remaining protoporphyrin in the intestine undergoes fecal excretion. Protoporphyrin is insoluble and hence unavailable for renal excretion. In EPP, subnormal biotransformation of protoporphyrin into heme results in accumulation of protoporphyrin in hepatocytes.
Since FECH deficiency is associated with increased concentrations of protoporphyrin in erythrocytes, plasma, skin and liver, retention of protoporphyrin in skin predisposes to acute photosensitivity. As a result of absorption of ultraviolet light (that is, wavelengths less than 400 nm) by protoporphyrin in plasma and erythrocytes when blood circulates through the dermal vessels, free radicals are formed, erythrocytes become unstable and injury to the skin is induced.
A significant increase in the hepatobiliary excretion on protoporphyrin can damage the liver through both cholestatic phenomena and oxidative stress predisposing to hepatobiliary disease of varying degrees of severity
Diagnosis
EPP is generally suspected by the presence of acute photosensitivity of the skin and can be confirmed by detection of a plasmatic fluorescence peak at 634 nm. It is also useful to find increased levels of protoporphyrin in feces and the demonstration of an excess of free protoporphyrin in erythrocytes.
Screening for FECH mutation on one allele or aminolevulinic acid synthase 2 gain-of-function mutation in selected family members may be useful, especially in genetic counseling.
Liver biopsy confirms hepatic disease in EPP by the presence of protoporphyrin deposits in the hepatocytes that can be observed as a brown pigment within the biliary canaliculi and the portal macrophages. Macroscopically, the cirrhotic liver can have a black color due to protoporphyrin deposits. Using polarized light the characteristic Maltese cross shape of birefringent crystalline pigment deposits is found. The examination of liver tissue under a Wood’s lamp reveals a red fluorescence due to protoporphyrin. Liver biopsy is not helpful for estimation of prognosis of liver disease.
Treatment and prognosis
There is no cure for this disorder; however, symptoms can usually be managed by limiting exposure to daytime sun and fluorescent lights. Protective clothing is also very helpful. Since the photosensitivity results from light in the visible spectrum, most sunscreens (with the exception of light-reflecting substances such as zinc oxide) are of little use. Some individuals may decrease their sun sensitivity with daily doses of beta carotene, though a recent meta analysis of carotene treatment has called its effectiveness into question. Some patients gradually build a protective layer of melanin by regularly exposing themselves for short times to ultraviolet radiation.
Window films which block UV and visible light up to 450 nm can provide relief from symptoms if applied to the patient's automobile and home windows.
EPP is considered one of the least severe of the porphyrias. Unless there is liver failure, it is not a life-threatening disease.
Approved therapies
The only approved medicine to treat EPP is afamelanotide, developed by Australian-based Clinuvel Pharmaceuticals and approved by the European Commission in December 2014 for treatment or prevention of phototoxicity in adult patients with EPP. It is marketed under the name Scenesse.
Off-label use
Several drugs are used off label by patients with EPP:
Bone marrow transplantation, liver transplantation, acetylcysteine, extracorporeal albumin dialysis, parenteral iron and transfusion of erythrocytes are alternative plans for treatment of EEP.
Epidemiology
Case reports suggest that EPP is prevalent globally. The prevalence has been estimated somewhere between 1 in 75,000 and 1 in 200,000 however it has been noted that the prevalence of EPP may be increasing due to a better understanding of the disease and improved diagnosis. An estimated 5,000-10,000 individuals worldwide have EPP. EPP is considered the most common form of porphyria in children. The prevalence in Sweden has been published as 1:180,000.
History
Erythropoietic protoporphyria was first described in 1953 by Kosenow and Treibs and completed in 1960 by Magnus et al. at the St John's Institute of Dermatology in London.
Popular culture
In the 9th episode of season 3 of House entitled Finding Judas, the primary patient is a young girl who is ultimately diagnosed with erythropoietic protoporphyria.
In series 14 episode 26 of Casualty entitled Seize the Night, one of the patients admitted to the department was a young girl who had erythropoietic protoporphyria. She got brought in after being hit by a car.
The June 14, 2015 episode of Dateline NBC entitled Out of the Shadows was devoted to the topic of children with erythropoietic protoporphyria.