
Specialty oncology ICD-O M9717/3 | ICD-10 C86.2 | |
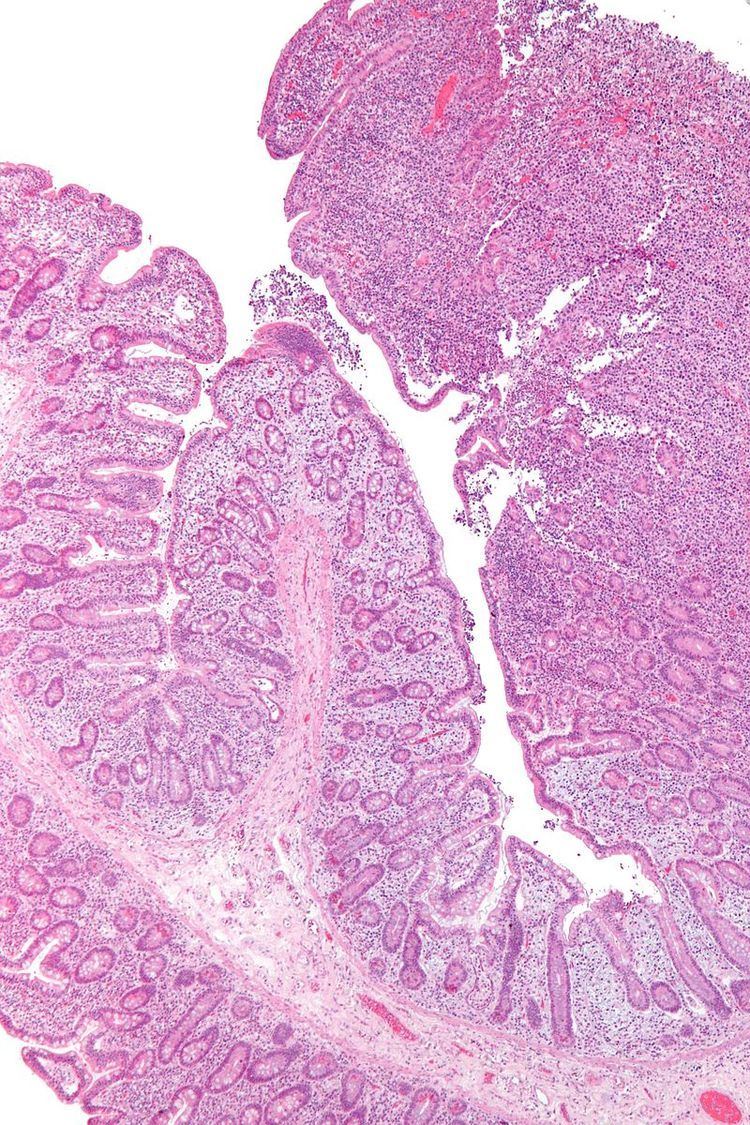 | ||
Enteropathy-associated T-cell lymphoma (EATL), also enteropathy-type T-cell lymphoma (ETTL), is a type of T-cell lymphoma that affects the small intestine. It is the most common primary gastrointestinal T-cell lymphoma, arising from the T cells that are found between the cells that line the small intestinal (brush border cells or small intestinal epithelial cells). These cancerous T-cells are a possible consequence of refractory cases of coeliac disease or in chronic, untreated cases in genetically susceptible individuals.
Contents
Epidemiology
EATL is most frequent in Europe, where it represents 9.4% of all peripheral T cell lymphomas. Association with celiac disease is consistently demonstrated in only 30% of patients. The global incidence of this lymphoma is rare, being about 0.5 to 1 per million.
Classification
EATL can be classified as an extranodal peripheral T cell lymphoma, a category it shares with hepatosplenic T cell lymphoma and panniculitic T cell lymphoma. It can be further classified in type I and II EATL.
Genetics
Enteropathy associated T-cell lymphoma (EATL) is environmentally induced as a result of the consumption of Triticeae glutens (e.g. wheat gluten). In gluten-sensitive individuals with EATL, 68% are homozygotes of the DQB1*02 subtype at the HLA-DQB1 locus. (See Coeliac Disease, HLA-DQ, HLA DR3-DQ2) A DQ isoform that appears to be responsible for EATL in the overwhelming number of cases is highly effective at presenting a proteolytically protected region of α2-gliadin to T-cells, constant over-stimulation of T-cell eventually results in neoplastic growth. EATL typically appears after the 4th decade of life, within 3 years of coeliac disease diagnosis or in undiagnosed coeliacs. In treated coeliacs, EATL may be preceded by refractory coeliac disease 1(RCD1) or, prominently, refractory celiac disease 2 (RCD2), in which EATL is a frequent outcome. Refractory coeliac disease is no longer favorably responsive to wheat-gluten abstinence. Beyond the RCD1 stage, many drugs are not effective, and undetected coeliac disease leading to de novo EATL generally has a poor outcome.
The genetic association with celiac disease and HLA loci defines type I EATL. Type II doesn´t show these associations and frequently presents with bulky disease.
Early recognition of coeliac disease, particularly with a focus on DQ2 homozygotes and in affected family members, is the only effective prevention, though bone marrow transplant was suggested as a treatment during early RCD2.
Staging
Bone marrow involvement is rare in this disease.
Treatment
In certain eligible patients, a conditioning regimen of high-dose chemotherapy followed by an autologous stem cell transplant may be used to extend a period of first complete remission. Likewise, a recent study suggests that high dose therapy and autologous stem cell transplantation results in favorable outcomes for elderly patients with Non-Hodgkin's Lymphoma.
Prognosis
According to the Peripheral T-Cell Lymphoma Project, median overall survival is ten months, while median failure-free survival is only six months . The peripheral index for T-cell lymphoma is useful in defining prognosis for enteropathy-associated T-cell lymphoma. Among the most influential prognostic factors is bulky disease, defined by a tumor mass greater than 5 cm.
Autologous stem cell transplantation is feasible for selected patients with enteropathy-associated T-cell lymphoma and can yield durable disease control in a significant proportion of these patients. One study found a trend for better survival in patients transplanted in first complete or partial remission at four years (66% vs. 36%; P = .062).