
Rank Species | Phylum Platyhelminthes | |
 | ||
Scientific name Echinococcus multilocularis Similar Echinococcus, Echinococcus granulosus, Tapeworms, Dipylidium caninum, Dipylidium | ||
Echinococcus multilocularis is a cyclophyllid tapeworm that, along with some other members of the Echinococcus genus (especially E. granulosus), produces the disease known as echinococcosis in certain terrestrial mammals, including wolves, foxes, jackals, coyotes, domestic dogs and humans. Unlike E. granulosus, E. multilocularis produces many small cysts (also referred to as locules) that spread throughout the internal organs of the infected animal. Ingestion of these cysts, usually by a canid eating an infected rodent, results in a heavy infestation of tapeworms.
Contents
Signs and symptoms
People infected with E. multilocularis may be asymptomatic for many years. Following the asymptomatic period of this disease, common symptoms are headache, nausea, vomiting, abdominal pain. Jaundice is rare, but hepatomegaly is a common physical finding.
Life cycle
The life cycle of E. multilocularis involves a primary or definitive host and a secondary or intermediate host, each harboring different life stages of the parasite.
Foxes, coyotes, domestic dogs, and other canids are the definitive hosts for the adult stage of the parasite. Cats may also be involved. The head of the tapeworm attaches to the intestinal mucosa by hooks and suckers. It then produces hundreds of microscopic eggs, which are dispersed through the feces.
Wild rodents such as mice serve as the intermediate host. Eggs ingested by rodents develop in the liver, lungs and other organs to form multilocular cysts. Humans could also become an intermediate host by handling infected animals or ingesting contaminated food, vegetable, and water. The life cycle is completed after a fox or canine consumes a rodent infected with cysts. Larvae within the cyst develop into adult tapeworms in the intestinal tract of the definitive host.
Except in rare cases where infected humans are eaten by canines, humans are a dead-end or incidental host (an intermediate host that does not allow transmission to the definitive host) for E. multilocularis.
- adult worm present in intestine of definitive host
- eggs passed in feces, ingested by humans or intermediate host
- onchosphere penetrates intestinal wall, carried via blood vessels to lodge in organs
- hydatid cysts develop in liver, lungs, brain, heart
- protoscolices (hydatid sand) ingested by definitive host
- ingested protoscolices attach to small intestine and develops into adult worm
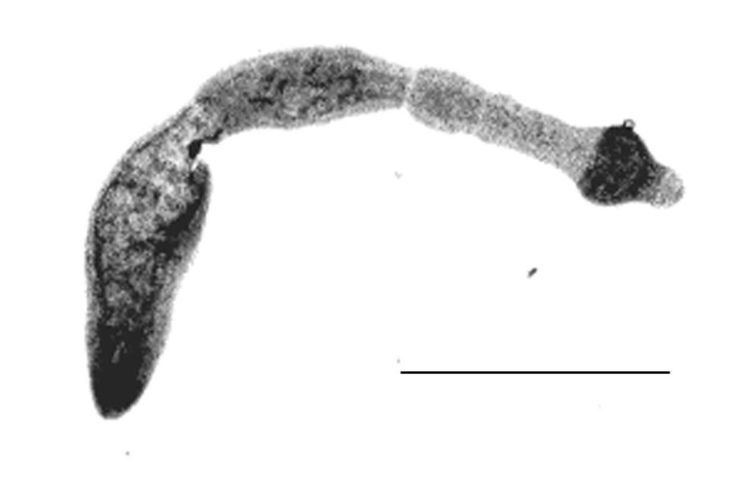
Morphology
The adult parasite is a small tapeworm that is 3- 6mm long, and lives in the small intestine of canines. The segmented worm contains a scolex with suckers and hooks that enable attachment to the mucosal wall, since tapeworms do not have a digestive tract. A short neck connects the head to three proglottids, the body segment of the worm which contains the eggs to be excreted in the feces.
Diagnosis
Serological and imaging tests are commonly used to diagnose this disease. Frequently used serological tests include antibody tests, ELISA and indirect hemaglutination (IHA). Also, an intradermal allergic reaction test (Casoni test) has also been used to diagnose patients. Imaging tests include: X-rays, cat scans, MRI, and ultrasound.
Disease staging
Alveolar echinococcosis (AE) is a highly lethal helminthic disease in humans, caused by the larval form of the parasitic tapeworm E. multilocularis. The disease represents a serious public threat in China, Siberia, and central Europe. However, since the 1990s, the prevalence of the disease seems to be increasing in Europe, not only in the historically endemic areas but its neighboring regions. AE primarily affects the liver by inducing a hepatic disorder similar to liver cancer, therefore becoming extremely dangerous and difficult to diagnose. If the infection metastasizes, it may spread to any other organ and could be lethal if not treated. The most common treatment for AE is to surgically remove the parasite. Since it is difficult and not always possible to remove the entire parasite, medicine such as Albendazole is utilized to keep the cyst from growing back.
Guided by the Tumor-Node-Metastasis (TNM) system of liver cancer, the European Network for Concerted Surveillance of Alveolar Echinococcosis and the World Health Organization Informal Working Group on Echinococcosis, a clinical classification system has been proposed. This classification system has been designated as the "PNM" system (P = parasitic mass, N = involvement of neighboring organs, M = metastasis). The system was developed by a retrospective analysis of records from 97 patients treated in France and Germany (2 treatment centers). Amongst other characteristics, the system takes into consideration the localization of the parasite in the liver, the extent of lesion involvement, regional involvement, and metastasis.
Treatment
If no specific therapy is initiated, in 94% of patients the disease is fatal within 10–20 years following diagnosis.
Epidemiology
The incidence of human infestation with E. multilocularis and disease is increasing in urban areas, as wild foxes (an important reservoir species of the sylvatic cycle) are migrating to urban and suburban areas and gaining closer contact with human populations. Also, restocking fox enclosures for fox hunting with infected animals spreads the disease. Children, health care workers and domestic animals are at risk of ingesting the cysts after coming into contact with the feces of infected wild foxes. Even with the improvement of health in developed/industrialized countries, the prevalence of alveolar echinococcosis (AE) did not decrease. On the contrary, incidents of AE have now also been registered in eastern European countries and sporadic incidences in other European countries.
The disease has extended its range in Europe in the last few decades. Still the infection is fairly rare. Between 1982 and 2000 a total of 559 cases were reported throughout Europe.
Recent findings indicate that E. multilocularis is likely expanding its range in the central region of the United States and Canada and that invasions of European strains might have occurred; the endemic presence of the parasite in urban areas and a recent human case in Alberta, Canada have been reported.