
Specialty oncology ICD-9-CM 8832/3 OMIM 607907 | ICD-10 C49 (ILDS C49.M24) ICD-O 8833/3 DiseasesDB 31601 | |
 | ||
Dermatofibrosarcoma protuberans (DFSP) is a very rare tumor. It is a rare neoplasm of the dermis layer of the skin, and is classified as a sarcoma. There is only about one case per million per year. DFSP is a fibrosarcoma, more precisely a cutaneous soft tissue sarcoma. In many respects, the disease behaves as a benign tumor, but in 2–5% of cases it can metastasize, so it should be considered to have malignant potential. It occurs most often in adults in their thirties; it has been described congenitally, in children, and the elderly. It accounts for approximately 2–6% of soft tissue sarcoma cancers.
Contents
Diagnosis
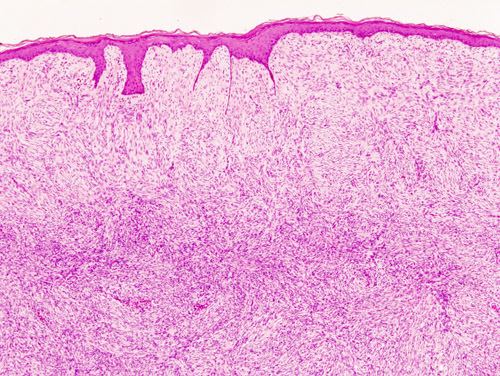
Dermatofibrosarcoma protuberans is diagnosed with a biopsy, when a portion of the tumor is removed for examination. In order to ensure that enough tissue is removed to make an accurate diagnosis, the initial biopsy of a suspected DFSP is usually done with a core needle or a surgical incision.
Presentation
Dermatofibrosarcoma protuberans can begin as a minor firm area of skin most commonly about to 1 to 5 cm in diameter. It can resemble a bruise, birthmark, or pimple. It is a slow growing tumor and is usually found on the torso but can also be found on the arms, legs, head and neck. About 90% of DFSPs are low grade sarcomas. About 10% are mixed; they contain a high-grade sarcomatous component (DFSP-FS); therefore, they are considered to be intermediate-grade sarcomas. DFSPs rarely lead to a metastasis (fewer than 5% do metastasise), but DFSPs can recur locally. DFSPs most often arise in patients who are in their thirties, but sometimes have been described in children or the elderly.
Pathophysiology
More than 90% of DFSP tumors have the chromosomal translocation t(17;22). The translocation fuses the collagen gene (COL1A1) with the platelet-derived growth factor (PDGF) gene. The fibroblast, the cell of origin of this tumor, expresses the fusion gene in the belief that it codes for collagen. However the resulting fusion protein is processed into mature platelet-derived growth factor which is a potent growth factor. Fibroblasts contain the receptor for this growth factor. Thus the cell "thinks" it is producing a structural protein, but it actually produces a self-stimulatory growth signal. The cell divides rapidly and a tumor forms.
The tissue is often positive for CD34.
Treatment
Treatment is primarily surgical, with chemotherapy and radiation therapy sometimes used.
The NCCN guideline recommends CCPDMA or Mohs surgery for the best cure rate of DFSP. Mohs surgery can be extremely effective. It will remove the tumor and all related pathological cells without a wide-area excision that may overlook sarcoma cells that have penetrated muscle tissue.
The standard of care for patients with DFSP is surgery. Usually, complete surgical resection with margins of 2 to 4 cm (recommended) is performed. The addition of adjuvant radiotherapy (irradiation) improves local control in patients with close or positive margins during the surgery. A special surgical technique, the "Mohs micrographic surgery" (MMS), can be employed in patients with DFSP. MMS is technically possible if the DFSP is in an anatomically confined area. A high probability of cure of DFSP can be attained with MMS as long as the final margins are negative. Patients who have a recurrent DFSP can have further surgery, but the probability of adverse effects of surgery and/or metastasis is increased in these patients. The Mohs surgery is highly successful.
Imatinib is approved for treatment. As is true for all medicinal drugs that have a name that ends in "ib," imatinib is a small molecular pathway inhibitor; imatinib inhibits tyrosine kinase. It may be able to induce tumor regression in patients with recurrent DFSP, unresectable DFSP or metastatic DFSP. There is clinical evidence that imatinib, which inhibits PDGF-receptors, may be effective for tumors positive for the t(17;22) translocation.