
 | ||
There are many different methods of birth control, which vary in what is required of the user, side effects, and effectiveness. It is also important to note that not each type of birth control is ideal for each user. Outlined here are the different types of barrier methods, spermicides, or coitus interruptus that must be used at before every act of intercourse. Immediate contraception, like physical barriers, include diaphragms, caps, the contraceptive sponge, and female condoms may be placed several hours before intercourse begins (note that when using the female condom, the penis must be guided into place when initiating intercourse). The female condom should be removed immediately after intercourse, and before arising.[1] Some other female barrier methods must be left in place for several hours after sex. Depending on the form of spermicide used, they may be applied several minutes to an hour before intercourse begins. Additionally, the male condom should be applied when the penis is erect so that it is properly applied prior to intercourse.
Contents
- User dependence
- Side effects
- Sexually transmitted disease prevention
- Effectiveness calculation
- Effectiveness
- Cost and cost effectiveness
- References
With an insertion of an IUD (intrauterine device), female or male sterilization, or hormone implant, there is very little required of the user post initial procedure; there is nothing to put in place before intercourse to prevent pregnancy.[2] Intrauterine methods require clinic visits for installation and removal or replacement (if desired) only once every several years (5-12), depending on the device. This allows the user to be able to try and become pregnant if they so desire, upon removal of the IUD. Conversely, sterilization is a one-time, permanent procedure. After the success of surgery is verified (for vasectomy), no subsequent action is usually required of users.
Implants, such as Nexplanon, provide effective birth control for three years without any user action between insertion and removal of the implant. Insertion and removal of the Implant involves a minor surgical procedure. Oral contraceptives require some action every day. Other hormonal methods require less frequent action - weekly for the patch, twice a month for vaginal ring, monthly for combined injectable contraceptive, and every twelve weeks for the injection Depo-Provera. Fertility awareness-based methods require some action every day to monitor and record fertility signs. The lactational amenorrhea method (LAM) requires breast feeding at least every four to six hours.
User dependence
Different methods require different levels of diligence by users. Methods with little or nothing to do or remember, or that require a clinic visit less than once per year are said to be non-user dependent, forgettable or top-tier methods. Intrauterine methods, implants and sterilization fall into this category. For methods that are not user dependent, the actual and perfect-use failure rates are very similar.
Many hormonal methods of birth control, and LAM require a moderate level of thoughtfulness. For many hormonal methods, clinic visits must be made every three months to a year to renew the prescription. The pill must be taken every day, the patch must be reapplied weekly, or the ring must be replaced monthly. Injections are required every 12 weeks. The rules for LAM must be followed every day. Both LAM and hormonal methods provide a reduced level of protection against pregnancy if they are occasionally used incorrectly (rarely going longer than 4–6 hours between breastfeeds, a late pill or injection, or forgetting to replace a patch or ring on time). The actual failure rates for LAM and hormonal methods are somewhat higher than the perfect-use failure rates.
Higher levels of user commitment are required for other methods. Barrier methods, coitus interruptus, and spermicides must be used at every act of intercourse. Fertility awareness-based methods may require daily tracking of the menstrual cycle. The actual failure rates for these methods may be much higher than the perfect-use failure rates.
Side effects
Different forms of birth control have different potential side effects. Not all, or even most, users will experience side effects from a method.
The less effective the method, the greater the risk of the side-effects associated with pregnancy.
Minimal or no other side effects are possible with coitus interruptus, fertility awareness-based, and LAM. Some forms of periodic abstinence encourage examination of the cervix; insertion of the fingers into the vagina to perform this examination may cause changes in the vaginal environment. Following the rules for LAM may delay a woman's first post-partum menstruation beyond what would be expected from different breastfeeding practices.
Barrier methods have a risk of allergic reaction. Users sensitive to latex may use barriers made of less allergenic materials - polyurethane condoms, or silicone diaphragms, for example. Barrier methods are also often combined with spermicides, which have possible side effects of genital irritation, vaginal infection, and urinary tract infection.
Sterilization procedures are generally considered to have low risk of side effects, though some persons and organizations disagree. Female sterilization is a more significant operation than vasectomy, and has greater risks; in industrialized nations, mortality is 4 per 100,000 tubal ligations, versus 0.1 per 100,000 vasectomies.
After IUD insertion, users may experience irregular periods in the first 3–6 months with Mirena, and sometimes heavier periods and worse menstrual cramps with ParaGard. However, "ninety-nine percent of IUD users are pleased with them". A positive characteristic of IUDs is that fertility and the ability to become pregnant returns quickly once the IUD is removed.
Because of their systemic nature, hormonal methods have the largest number of possible side effects.
Sexually transmitted disease prevention
Male and female condoms provide significant protection against sexually transmitted diseases (STD) when used consistently and correctly. They also provide some protection against cervical cancer. Condoms are often recommended as an adjunct to more effective birth control methods (such as IUD) in situations where STD protection is also desired.
Other barrier methods, such as diaphragm may provide limited protection against infections in the upper genital tract. Other methods provide little or no protection against sexually transmitted diseases.
Effectiveness calculation
Failure rates may be calculated by either the Pearl Index or a life table method. A "perfect-use" rate is where any rules of the method are rigorously followed, and (if applicable) the method is used at every act of intercourse.
Actual failure rates are higher than perfect-use rates for a variety of reasons:
For instance, someone using oral forms of hormonal birth control might be given incorrect information by a health care provider as to the frequency of intake, or for some reason not take the pill one or several days, or not go to the pharmacy on time to renew the prescription, or the pharmacy might be unwilling to provide enough pills to cover an extended absence.
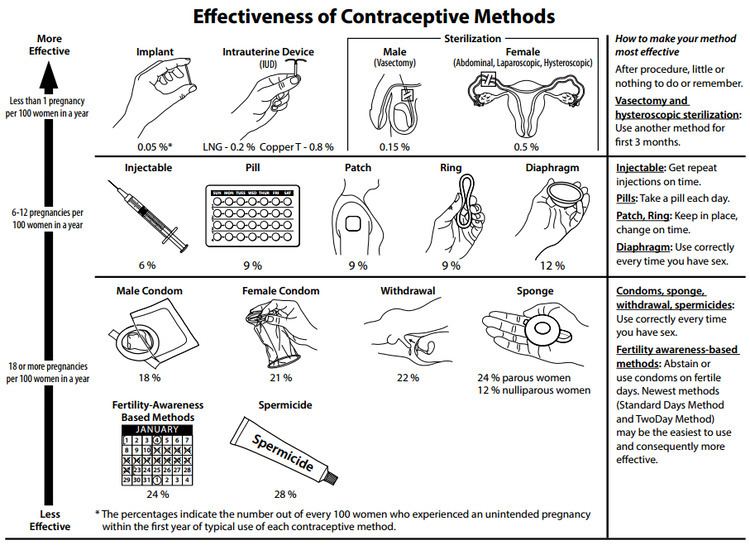
Effectiveness
The table below color codes the typical-use and perfect-use failure rates, where the failure rate is measured as the expected number of pregnancies per year per 100 women using the method:
In the user action required column, items that are non-user dependent (require action once per year or less) also have a blue background.
Some methods may be used simultaneously for higher effectiveness rates. For example, using condoms with spermicides the estimated perfect use failure rate would be comparable to the perfect use failure rate of the implant. However, mathematically combining the rates to estimate the effectiveness of combined methods can be inaccurate, as the effectiveness of each method is not necessarily independent, except in the perfect case.
If a method is known or suspected to have been ineffective, such as a condom breaking, emergency contraception (ECP) may be taken up to 72 to 120 hours after sexual intercourse. Emergency contraception should be taken shortly before or as soon after intercourse as possible, as its efficacy decreases with increasing delay. Although ECP is considered an emergency measure, levonorgestrel ECP taken shortly before sex may be used as a primary method for woman who have sex only a few times a year and want a hormonal method, but don’t want to take hormones all the time. Failure rate of repeated or regular use of LNG ECP is similar to rate for those using a barrier method.
This table lists the chance of pregnancy during the first year of use.
Cost and cost-effectiveness
Family planning is among the most cost-effective of all health interventions. Costs of contraceptives include method costs (including supplies, office visits, training), cost of method failure (ectopic pregnancy, spontaneous abortion, induced abortion, birth, child care expenses) and cost of side effects. Contraception saves money by reducing unintended pregnancies and reducing transmission of sexually transmitted infections. By comparison, in the US, method related costs vary from nothing to about $1,000 for a year or more of reversible contraception.
During the initial five years, vasectomy is comparable in cost to the IUD. Vasectomy is much less expensive and safer than tubal ligation.
Since ecological breastfeeding and fertility awareness are behavioral they cost nothing or a small amount upfront for a thermometer and / or training. Fertility awareness based methods can be used throughout a woman's reproductive lifetime.
Not using contraceptives is the most expensive option. While in that case there are no method related costs, it has the highest failure rate, and thus the highest failure related costs. Even if one only considers medical costs relating to preconception care and birth, any method of contraception saves money compared to using no method.
The most effective and the most cost-effective methods are long-acting methods. Unfortunately these methods often have significant up-front costs, requiring the user to pay a portion of these costs prevents some from using more effective methods. Contraception saves money for the public health system and insurers.