
Species Human Entrez 94025 | Human Mouse Ensembl ENSG00000181143 | |
 | ||
Aliases MUC16, CA125, mucin 16, cell surface associated External IDs OMIM: 606154 HomoloGene: 133291 GeneCards: MUC16 | ||
CA-125 (cancer antigen 125, carcinoma antigen 125, or carbohydrate antigen 125) also known as mucin 16 or MUC16 is a protein that in humans is encoded by the MUC16 gene. MUC16 is a member of the mucin family glycoproteins. CA-125 has found application as a tumor marker or biomarker that may be elevated in the blood of some patients with specific types of cancers, or other conditions that are benign.
Contents
Structure
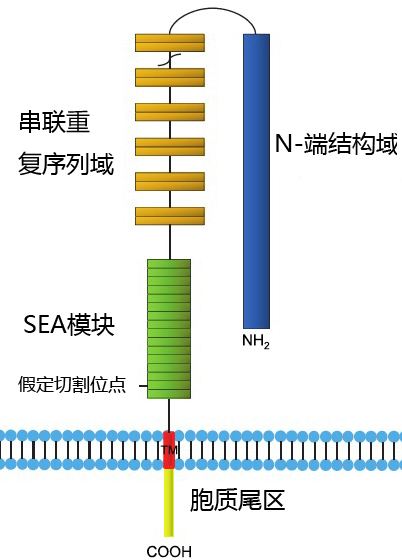
Mucin 16 is a membrane associated mucin that possesses a single transmembrane domain. A unique property of MUC16 is its large size. MUC16 is more than twice as long as MUC1 and MUC4 and contains about 22,000 amino acids, making it the largest membrane-associated mucin.
MUC16 is composed of three different domains:
The N-terminal and tandem repeat domains are both entirely extracellular and highly O-glycosylated. All mucins contain a tandem repeat domain that has repeating amino acid sequences high in serine, threonine and proline. The C-terminal domain contains multiple extracellular SEA (sea urchin sperm protein, enterokinase, and agrin) modules, a transmembrane domain, and a cytoplasmic tail. The extracellular region of MUC16 can be released from the cell surface by undergoing proteolytic cleavage. MUC16 is thought to be cleaved at a site in the SEA modules.
Function
MUC16 is a component of the ocular surface (including the cornea and conjunctiva), the respiratory tract and the female reproductive tract epithelia. Since MUC16 is highly glycosylated it creates a hydrophilic environment that acts as a lubricating barrier against foreign particles and infectious agents on the apical membrane of epithelial cells. Also, the cytoplasmic tail of MUC16 has been shown to interact with cytoskeleton by binding members of the ERM protein family. The expression of mucin 16 has been shown to be altered in dry eye, cystic fibrosis, and several types of cancers.
As a biomarker
CA-125 is the most frequently used biomarker for ovarian cancer detection. Medical societies including American Congress of Obstetricians and Gynecologists recommend against women with average risk of ovarian cancer having routine CA-125 screening or other screening for this cancer. Reasons for this include evidence that ambiguous test results are more likely to lead to further invasive, harmful, and unnecessary health care than they are likely to detect ovarian cancer in women who are at average risk of developing it.
Around 90% of women with advanced ovarian cancer have elevated levels of CA-125 in their blood serum, making CA-125 a useful tool for detecting ovarian cancer after the onset of symptoms. Monitoring CA-125 blood serum levels is also useful for determining how ovarian cancer is responding to treatment (with the duration of disease-free survival correlating with the rate of fall of CA-125) and for predicting a patient’s prognosis after treatment. This is because the persistence of high levels of CA-125 during therapy is associated with poor survival rates in patients. Also, an increase in CA-125 levels within individuals in a remission is a strong predictor of the recurrence of ovarian cancer. Indeed, a rising CA-125 level may precede clinical evidence of disease relapse by an interval of 3 to 6 months.
Prognosis relates to both the initial and post-treatment CA-125 values. A preoperative value >65 U/mL suggests a poor prognosis. Persistent elevations following chemotherapy indicate a poor prognosis. The half-life of CA-125 after chemotherapy correlates with prognosis (patients with CA-125 half-life <20 days show improved survival). Time-to-normalization (rate of fall of CA-125) affects prognosis with more rapid normalization within 3 cycles of chemotherapy correlating with improved survival.
In April 2011 the UK's National Institute for Health and Clinical Excellence (NICE) recommended that women with symptoms that could be caused by ovarian cancer should be offered a CA-125 blood test. The aim of this guideline is to help diagnose the disease at an earlier stage, when treatment is more likely to be successful. Women with higher levels of the marker in their blood would then be offered an ultrasound scan to determine whether they need further tests.
In one case, elevated serum levels of CA-125 were observed in a male patient with IgE myeloma, however more cases are needed to determine the clinical significance of CA-125 in myeloma.
Early detection of ovarian cancer
The potential role of CA-125 for the early detection of ovarian cancer is controversial and has not yet been adopted for widespread screening efforts in asymptomatic women. The major issues with using the CA-125 biomarker are its lack of sensitivity, particularly for detecting early stages of ovarian cancer, and its lack of specificity, especially in premenopausal women. These limitations mean that CA-125 testing often gives false positives for ovarian cancer and puts patients through unnecessary further screening (sometimes including surgery) and anxiety. Also, these limitations mean that many women with early stage ovarian cancer will receive a false negative from CA-125 testing and not get further treatment for their condition.
Specificity and sensitivity
CA-125 has limited specificity for ovarian cancer because elevated CA-125 levels can be found in individuals without ovarian cancer. For example, while CA-125 is best known as a marker for ovarian cancer, it may also be elevated in other cancers, including endometrial cancer, fallopian tube cancer, lung cancer, breast cancer and gastrointestinal cancer. CA-125 may also be elevated in a number of relatively benign conditions, such as endometriosis, several diseases of the ovary, menstruation and pregnancy. It also tends to be elevated in the presence of any inflammatory condition in the abdominal area, both cancerous and benign, as well as in cirrhosis and diabetes mellitus. Thus, CA-125 testing is not perfectly specific for ovarian cancer and often results in false positives.
The specificity of CA-125 is particularly low in premenopausal women because many benign conditions that cause fluctuations in CA-125 levels, such as menstruation, pregnancy, and pelvic inflammatory disease, are seen in this population.
CA-125 testing is also not perfectly sensitive for detecting ovarian cancer because not every patient with cancer will have elevated levels of CA-125 in their blood. For example, 79% of all ovarian cancers are positive for CA-125, whereas the remainder do not express this antigen at all. Also, only about 50% of patients with early stage ovarian cancer have elevated CA-125 levels, meaning that CA-125 has particularly poor sensitivity for ovarian cancer before the onset of symptoms. Poor sensitivity means that the use of CA-125 to detect ovarian cancer (especially in early stages of disease) can frequently lead to false negatives. Patients that receive false negatives are unlikely to seek further treatment for their disease.
Ranges in ovarian cancer
While this test is not generally regarded as useful for large scale screening by the medical community, a high value may be an indication that the woman should receive further diagnostic screening or treatment. Normal values range from 0 to 35 (U/mL). Elevated levels in post-menopausal women are usually an indication that further screening is necessary. In pre-menopausal women, the test is less reliable as values are often elevated due to a number of non-cancerous causes, and a value above 35 is not necessarily a cause for concern.
In a patient who is clinically selected for testing due to the presence of an adnexal/pelvic mass, CA-125 has great utility to differentiate benign from malignant processes. In a post-menopausal woman with a palpable adnexal mass and CA-125 level greater than 65 U/mL, the positive predictive value is >95% for ovarian malignancy. In patients who are not as carefully selected clinically, the utility of this test decreases, thus highlighting the need for careful clinical scrutiny.
Role in cancer
MUC16 (CA-125) has been shown to play a role in advancing tumorigenesis and tumor proliferation by several different mechanisms.
Immune system evasion
One way that MUC16 helps the growth of tumors is by suppressing the response of natural killer cells, thereby protecting cancer cells from the immune response. Further evidence that MUC16 can protect tumor cells from the immune system is the discovery that the heavily glycosylated tandem repeat domain of MUC16 can bind to galectin-1 (an immunosuppressive protein).
Metastatic invasion
MUC16 is also thought to participate in cell-to-cell interactions that enable the metastasis of tumor cells. This is supported by evidence showing that MUC16 binds selectively to mesothelin, a glycoprotein normally expressed by the mesothelial cells of the peritoneum (the lining of the abdominal cavity). MUC16 and mesothelin interactions are thought to provide the first step in tumor cell invasion of the peritoneum.
Mesothelin has also been found to be expressed in several types of cancers including mesothelioma, ovarian cancer and squamous cell carcinoma. Since mesothelin is also expressed by tumor cells, MUC16 and mesothelial interactions may aid in the gathering of other tumor cells to the location of a metastasis, thus increasing the size of the metastasis.
Induced motility
Evidence suggests that expression of the cytoplasmic tail of MUC16 enables tumor cells to grow, promotes cell motility and may facilitate invasion. This appears to be due to the ability of the C-terminal domain of MUC16 to facilitate signaling that leads to a decrease in the expression of E-cadherin and increase the expression of N-cadherin and vimentin, which are expression patterns consistent with epithelial-mesenchymal transition.
Chemotherapy resistance
MUC16 may also play a role in reducing the sensitivity of cancer cells to drug therapy. For example, overexpression of MUC16 has been shown to protect cells from the effects of genotoxic drugs, such as cisplatin.
Discovery
CA-125 was initially detected using the murine monoclonal antibody designated OC125. Robert Bast, Robert Knapp and their research team first isolated this monoclonal antibody in 1981. The protein was named “cancer antigen 125” because OC125 was the 125th antibody produced against the ovarian cancer cell line that was being studied.