
Specialty hematology ICD-9-CM 287.1 DiseasesDB 1356 | ICD-10 D69.1 OMIM 231200 eMedicine ped/230 | |
 | ||
Bernard–Soulier syndrome (BSS), also called hemorrhagiparous thrombocytic dystrophy, is a rare autosomal recessive coagulopathy (bleeding disorder) that causes a deficiency of glycoprotein Ib (GpIb), the receptor for von Willebrand factor The incidence of BSS is estimated to be less than 1 case per million persons, based on cases reported from Europe, North America, and Japan. BSS is a giant platelet disorder, meaning that it is characterized by abnormally large platelets
Contents
Signs and symptoms
Bernard–Soulier syndrome often presents as a bleeding disorder with symptoms of:
Genetics
In regards to mechanism, there are three genes:GP1BA, GP1BB and GP9 that are involved (due to mutations) These mutations do not allow GPIb-IX-V complex to bind to the von Willebrand factor, which in turn is what would help platelets adhere to a site of injury which eventually helps stop bleeding.
Diagnosis
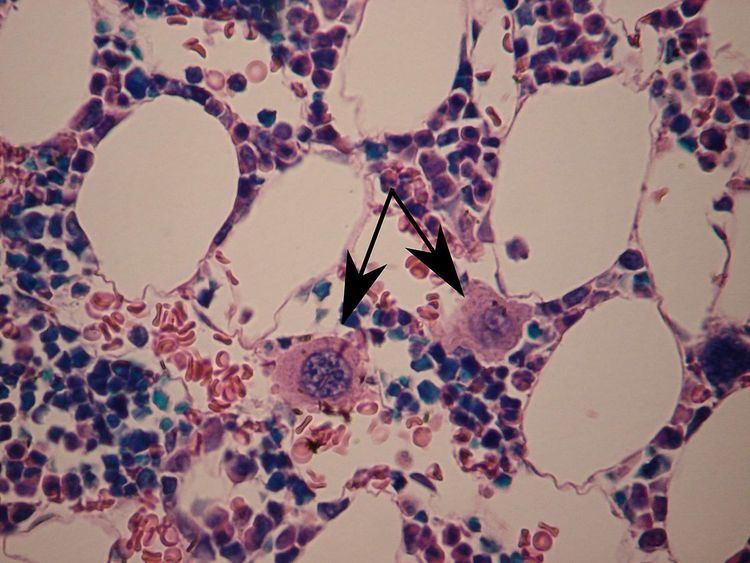
In terms of diagnosis Bernard–Soulier syndrome is characterized by prolonged bleeding time, thrombocytopenia, increased megakaryocytes, and enlarged platelets, Bernard–Soulier syndrome is associated with quantitative or qualitative defects of the platelet glycoprotein complex GPIb/V/IX. The degree of thrombocytopenia may be estimated incorrectly, due to the possibility that when the platelet count is performed with automatic counters, giant platelets may reach the size of red blood cells. The large platelets and low platelet count in BSS are seemingly due to the absence of GPIbα and the filamin A binding site that links the GPIb-IX-V complex to the platelet membrane skeleton.
Differential diagnosis
The differential diagnosis for Bernard–Soulier syndrome includes both Glanzmann thrombasthenia and pediatric Von Willebrand disease. BSS platelets do not aggregate to ristocetin, and this defect is not corrected by the addition of normal plasma, distinguishing it from von Willebrand disease.
Treatment
In terms of treatment/management, bleeding events can be controlled by platelet transfusion. Most heterozygotes, with few exceptions, do not have a bleeding diathesis.BSS presents as a bleeding disorder due to the inability of platelets to bind and aggregate at sites of vascular endothelial injury. In the event of an individual with mucosal bleeding tranexamic acid can be given.
The affected individual may need to avoid contact sports and medications such as aspirin, which can increase the possibility of bleeding.A potential complication is the possibility of the individual producing antiplatelet antibodies
Prevalence
The frequency of Bernard–Soulier syndrome is approximately 1 in 1,000,000 people. The syndrome, identified in the year 1948, is named after Dr. Jean Bernard and Dr. Jean Pierre Soulier.