
 | ||
The abdominal exam, in medicine, is performed as part of a physical examination, or when a patient presents with abdominal pain or a history that suggests an abdominal pathology.
Contents
- Purpose
- Positioning and environment
- Inspection
- Auscultation
- Palpation
- Percussion
- Other and special maneuvers
- References
The abdominal exam has conventionally been split into different stages:
Purpose
According to Mosby's, "The abdominal exam is performed as part of the comprehensive physical examination or when a patient presents with signs of symptoms of an abdominal disease process." In other words, your doctor will often perform an abdominal exam as part of a routine examination. However, your doctor might perform additional tests if your doctor feels that you might have an abdominal disease.
Positioning and environment
A suggested position is for the patient to be supine (on their back), with their arms to their sides. The patient should be placed in an environment with good lighting, and should be draped with towels or sheets to preserve privacy and warmth
Although physicians have had concern that giving patients pain medications during acute abdominal pain may hinder diagnosis and treatment, separate systematic reviews by the Cochrane Collaboration and the Rational Clinical Examination refute this.
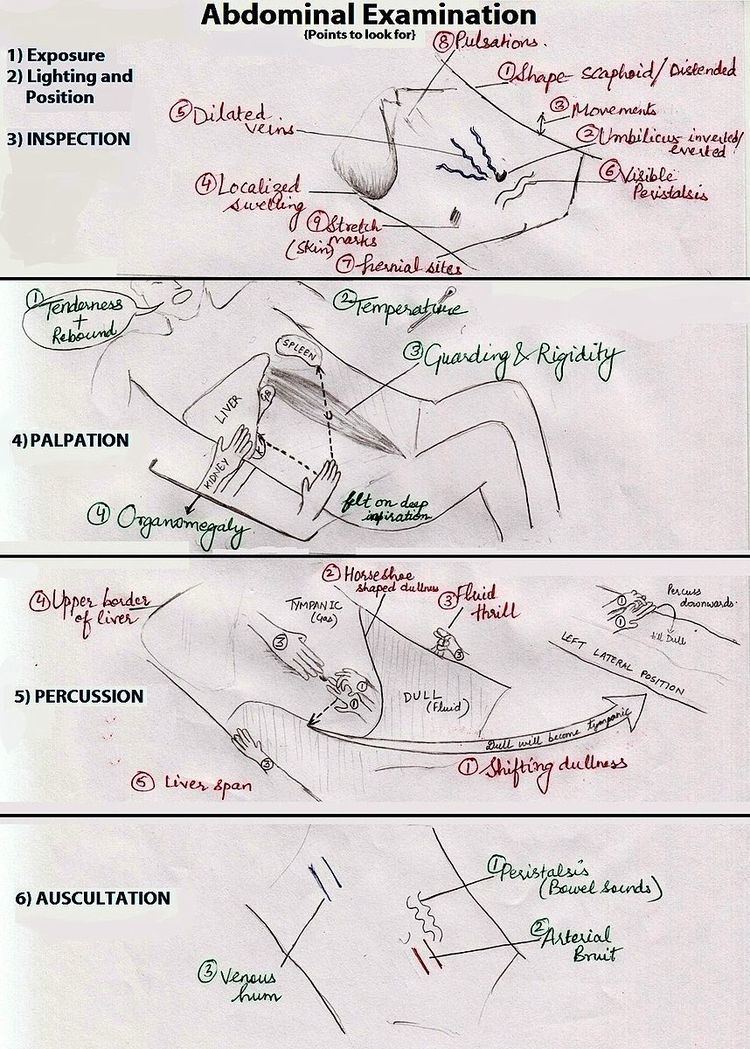
Inspection
The abdominal exam typically begins a visual examination of the abdomen. Some common things an examiner might look for are:
In addition, a doctor might look/check for specific signs of disease, such as:
Auscultation
Auscultation refers to the use of a stethoscope by the examiner to listen to sounds from the abdomen.
Unlike other physical exams, auscultation is performed prior to percussion or palpation, because both might alter abdominal sounds.
Some controversy exists as to the length of time required to confirm or exclude bowel sounds, with suggested durations up to five minutes. Bowel obstruction may present with grumbling bowel sounds or high-pitched noises. Absence of sounds may be caused by peritonitis.
The examiner also typically listens to the two renal arteries for bruits by listening in each upper quadrant, adjacent to and above the umbilicus. Bruits heard in the epigastrium that are confined to systole are considered normal.
Palpation
The examiner typically palpates all nine areas of the patient's abdomen. This is typically performed twice, lightly and then deeply.
On light palpation, the examiner tests for any palpable mass, rigidity, or pain.
On deep palpation, the examiner is testing for and organomegaly, including enlargement of the liver and spleen.
Reactions that may indicate pathology include:
Percussion
The examiner, mindful of areas of discomfort, begins by palpating areas of no pain. Percussion is performed by knocking the middle finger against the phalanx of the middle finger of the opposing hand, which rests against the surface of the abdomen in each of the nine areas tested. Percussion can elicit a painful response in the patient, and may also reveal whether there is abnormal levels of fluid in the abdomen. Organomegaly may also be noted, including gross splenomegaly (enlargement of the spleen), hepatomegaly (enlargement of the liver), and urinary retention.
The examiner, when percussing for organomegaly, percusses in a particular manner:
Examination of the spleen
Other and special maneuvers
Special manevures may also be performed, to elicit signs of specific diseases. These include