
 | ||
Pressure-controlled intermittent coronary sinus occlusion (also known as PICSO), is a procedure utilized to enhance restoration of blood flow to the microcirculation in heart tissue following a myocardial infarction. PICSO has a dual therapeutic potential first for myocardial salvage and second for tissue regeneration. In a meta-analysis of preclinical studies a significant reduction of infarct size of about 30% as compared to controls was observed. Pilot clinical studies of PICSO in acute myocardial infarction confirmed an event free survival of patients indicating a significant risk reduction for reinfarction.
Contents
Conventional treatment
Myocardial infarction (MI), or heart attack, occurs when a blood clot forms around a plaque already obstructing flow in coronary arteries preventing proper blood supply. Total occlusion of a coronary artery is the consequence of a plaque rupture and forming a blood clot disrupting blood flow. This leads to a risk zone with rapid loss of oxygen delivery, deprivation of nutritive flow to the heart leading to necrosis of the myocardium known as MI. Myocardial infarctions are graded according to severity: The less severe type is Non ST-segment Elevated Myocardial infarction (NSTEMI) with deprivation of flow occurring only in the subendocardium. ST-Segment Elevation Myocardial Infarction (STEMI) is the severe type. Here the damage is transmural with a completely blocked coronary artery. Although many occluded coronary arteries spontaneously reopen before the patient is treated with PPCI (primary percutaneous catheter interventions), the consequence of the arterial occlusion is a wave of necrosis of the heart muscle within the deprived area dependent of the occlusion time of a major coronary artery Despiteand residual collateral flow. Current therapies in acute coronary syndrome (ACS) focus on the rapid reopening of the occluded coronary arteries (PPCI), but recently also the ischemic microcirculation became a therapeutic target. Coronary angioplasty (or primary percutaneous coronary intervention (PPCI)) has been used as a way to restore blood flow following an MI to the heart in order to prevent excessive damage to the tissue. This is the result of inadequate blood flow in the coronary microvasculature in spite of reopened large epicardial coronary arteries leaving myocardium insufficiently supported. Reduced myocardial blood flow causes in addition to necrosis apoptosis of sublethally injured tissue leading to reduced heart function and the potential of heart failure. This phenomenon is part of reperfusion injury (WP-Link), the damage of myocardium after reopening of major coronary arteries, accounts for 50% of the final infarct size after STEMI. Therefore, the therapeutic target before, during or after reopening of epicardial coronary arteries is the obstructed microcirculation. This obstruction of coronary microcirculation is the main target of PICSO clearing the coronary vasculature and restore nutritive flow by inducing washout in low flow or no flow areas.
The origin of coronary sinus intervention
The coronary sinus collects about 70% of the myocardial outflow. There are early concepts using the coronary sinus to access ischemic myocardium. First clinically useful techniques go back to the 1940s. In early experimental studies the consequences of elevated pressure in cardiac veins have been analyzed. The Beck´s procedure was an operation in patients with severe coronary artery disease long before modern cardiac surgery could be performed. By permanent occlusion of the coronary sinus and retroperfusion of arterial blood shunted into the coronary sinus, some patients improved and eased in their ischemic symptoms. Based on this concept and analyzing the side effects of permanent obstruction of coronary venous outflow a different concept (ICSO, pICSO, PICSO) was formulated. In the early 1980s, a scientific group headed by Werner Mohl invented ICSO as a temporal physiologically controlled outflow obstruction of flow in cardiac veins thus preventing known side effects in the coronary circulation. Intermittent coronary sinus occlusion (ICSO) used time dependent occlusion of the coronary sinus to redistribute flow within the cardiac veins, but also to allow sufficient time for venous outflow. A modification was pICSO, by observing the pressure within the coronary veins during occlusion. Pressure observed intermittent coronary sinus occlusion without automatic closed loop but with oberserver control of pressure increase was used in experimental infarction and showed substantial reduction of infarct size. pICSO was also used clinically presenting enhanced clot lysis and significant (30%) reduction of infarct size compared to lysis alone. In 1984 the concepts of ICSO and pICSO were replaced by PICSO. PICSO used physiologic parameters like venous pressure to establish a closed loop system for coronary sinus occlusion. This automation avoids inadequate duration of the coronary sinus occlusion with negative effects on the retroperfusion/drainage of the coronary sinus.
The importance of pressure control during coronary sinus occlusion
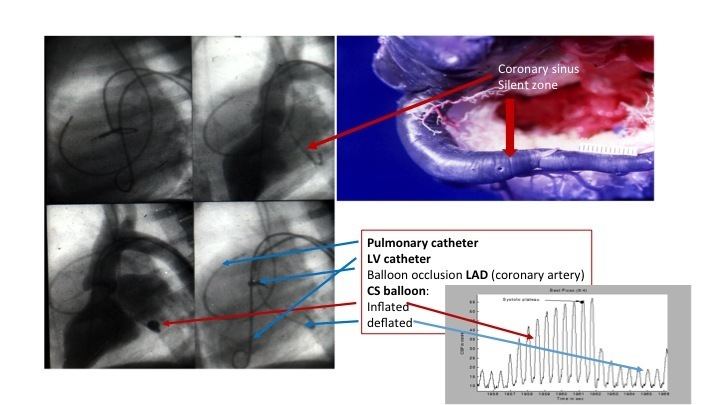
Outflow obstruction in cardiac veins by coronary sinus balloon occlusion fills the venous compartment and increases impedance to coronary artery inflow. This perfusion deficit is repaid by a hyperemic response initiated by the rapid fall of the elevated pressure after reopening of the balloon occlusion. Automated pressure control is therefore essential not only to optimize effectivity, but also to control these pressure responses in the coronary circulation. The continuous rise and fall of pressure gradients in the microvasculature is primarily of mechanical nature regaining access to deprived myocardium by excess perfusion and washout, but induces also the expression of vasoactive molecules. A balloon mounted catheter is inserted into the femoral vein along with a guide wire, and the catheter is fed into the coronary sinus. The coronary sinus is the primary vein of the heart and is responsible for collecting deoxygenated blood from a series of veins and delivering it to the right atrium. Once inside the coronary sinus, a console is responsible for orchestrating an inflation and deflation cycle of the balloon on the catheter. The blood pressure that occurs in the coronary sinus when it is blocked controls the cycle. The cycle is controlled by the pressure that occurs in the coronary sinus when it is blocked. The pressure increase redistributes flow into affected heart tissue thererby improving flow in the microcirculation. PICSO is a used therapy accompanying or as part of primary percutaneous coronary intervention (PPCI).
The intermittent action of coronary sinus pressure cycling, clear the microcirculation and remove cellular debris that may have accumulated during ischemia and reperfusion allowing better perfusion of otherwise no reflow zones. The commercially available PiCSO Impulse system automatically optimizes this effect and tunes (adjusts) the therapy to the size of the underperfused zone and the necessary hyperemic response during balloon deflation, the individual anatomical size of the vascular compartment thus preventing an unwanted increase of vascular resistance in global coronary circulation.
Salvage potential
The effects of PICSO were tested in several experimental and clinical studies. In one clinical study a five-year follow up indicated that PICSO has regenerative potential beyond its acute effects in the field of acute coronary syndrome (ACS). Significant reduction of infarct size was observed as compared to matched controls. The experiment also confirmed event free survival in patients with acute myocardial infarction and risk reduction for event free survival 5 years after the acute event. In addition the significance of myocardial salvage has been documented in several studies focusing on the "dose dependence" between optimized ICSO therapy and salvage.
Structural regenerative potential
Apart from the mechanism described above PICSO offers an unexpected regenerative potential. The mechanism is hypothesized to be the activation of vascular cells in cardiac veins in a threshold dependent way. New vasculature distal to an occluded coronary artery were described as long-term histologic changes of ischemic myocardium in presence of permanent occlusion of venous outflow in the Beck´s procedure. Neoangiogenesis caused by pulsatile pressure seems to be the mode of action described of structural recovery by the hypothesis "embryonic recall". Mohl describes in this hypothesis that intermittent pressure elevation results in equivalent signals normally effective during the embryonic development of the heart. Some of the same gene signals as in early heart development are activated via mechanotransduction effect of PICSO. Shear stress and pulsatile stretch on venous endothelium is responsible for inducing pathways upregulating vasoactive and cardioprotective molecules.