
ICD-10 C83.7 ICD-O M9687/3 | ICD-9-CM 200.2 OMIM 113970 | |
 | ||
Synonyms Burkitt's tumor, Burkitt's lymphoma, malignant lymphoma Burkitt's type Specialty Hematology and oncology | ||
Burkitt lymphoma is a cancer of the lymphatic system, particularly B lymphocytes found in the germinal center. It is named after Denis Parsons Burkitt, a surgeon who first described the disease in 1958 while working in equatorial Africa.
Contents
Classification
Currently, Burkitt lymphoma can be divided into three main clinical variants: the endemic, the sporadic, and the immunodeficiency-associated variants.
By morphology (i.e. microscopic appearance) or immunophenotype, it is almost impossible to differentiate these three clinical variants. Immunodeficiency-associated Burkitt lymphoma may demonstrate more plasmacytic appearance or more pleomorphism, but these features are not specific.
Malignant B cell characteristics
Normal B cells of a germinal center possess rearranged immunoglobulin heavy and light chain genes, and each isolated B cell possesses a unique IgH gene rearrangement. Since Burkitt lymphoma and other B-cell lymphomas are a clonal proliferative process, all tumor cells from one patient are supposed to possess identical IgH genes. When the DNA of tumor cells is analyzed using electrophoresis, a clonal band can be demonstrated, since identical IgH genes will move to the same position. On the contrary, when a normal or reactive lymph node is analyzed using the same technique, a smear rather than a distinct band will be seen. This technique is useful since sometimes benign reactive processes (e.g. infectious mononucleosis) and malignant lymphoma can be difficult to distinguish.
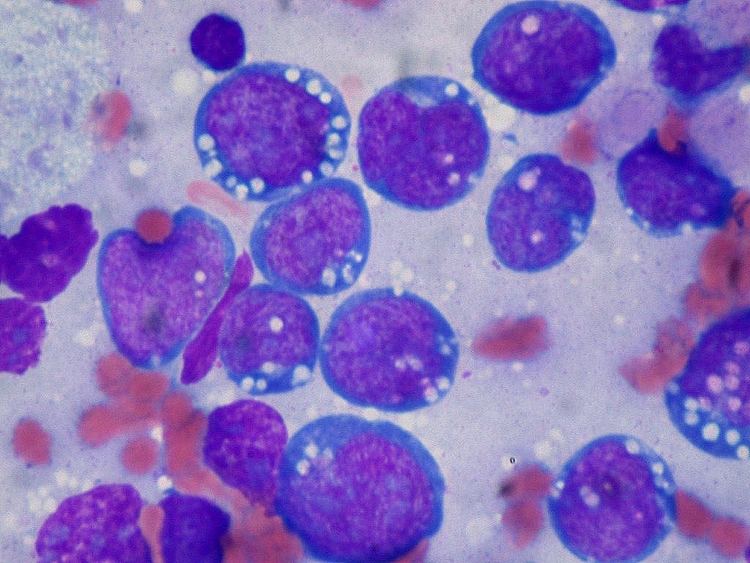
Microscopy
The tumor consists of sheets of a monotonous (i.e. similar in size and morphology) population of medium-sized lymphoid cells with high proliferative activity and apoptotic activity. The "starry sky" appearance seen under low power is due to scattered tingible body-laden macrophages (macrophages containing dead apoptotic tumor cells). The old descriptive term of "small non-cleaved cell" is misleading. The tumor cells are mostly medium in size (i.e. tumor nuclei size similar to that of histiocytes or endothelial cells). "Small non-cleaved cells" are compared to "large non-cleaved cells" of normal germinal center lymphocytes. Tumor cells possess small amount of basophilic cytoplasm with three to four small nucleoli. The cellular outline usually appears squared off.
Immunohistochemistry
The tumor cells in Burkitt lymphoma generally strongly express markers of B cell differentiation (CD20, CD22, CD19), as well as CD10 and BCL6. The tumour cells are generally negative for BCL2 and TdT. The high mitotic activity of Burkitt lymphoma is confirmed by nearly 100% of the cells staining positive for Ki67.
Genetics
All types of Burkitt lymphoma are characterized by dysregulation of the c-myc gene by one of three chromosomal translocations. This gene is found at 8q24.
Combined, the two less-common translocations, t(2;8)(p12;q24) and t(8;22)(q24;q11), account for the remaining 15% of cases not due to the t(8;14)(q24;q32) translocation.
MicroRNA expression
In 2014, it was described that short non-coding RNAs named microRNAs (miRNAs) have important functions in lymphoma biology. In malignant B cells miRNAs participate in pathways fundamental to B cell development like B cell receptor (BCR) signalling, B cell migration/adhesion, cell-cell interactions in immune niches, and the production and class-switching of immunoglobulins. MiRNAs influence B cell maturation, generation of pre-, marginal zone, follicular, B1, plasma and memory B cells.
Treatment
Treatment may be dose-adjusted EPOCH with rituximab or the modified Magrath regimen (R-CODOX-M/IVAC). Other protocols are CHOMP COPADM, hyper-CVAD, and the Cancer and Leukemia Group B (CALGB) 8811 regimen; these can be associated with rituximab. The effects of the chemotherapy, as with all cancers, depend on the time of diagnosis. With faster-growing cancers, such as Burkitt's, the cancer actually responds faster than with slower-growing cancers. This rapid response to chemotherapy can be hazardous to the patient, as a phenomenon called "tumor lysis syndrome" could occur. Close monitoring of the patient and adequate hydration is essential during the process. Since Burkitts lymphoma has high propensity to spread to the central nervous system (lymphomatous meningitis), intrathecal chemotherapy with methotrexate and/or ARA-C and/or prednisolone is given alongside with systemic chemotherapy.
Chemotherapy
Other treatments for Burkitt's lymphoma include immunotherapy, bone marrow transplants, stem cell transplant, surgery to remove the tumor, and radiotherapy.
Prognosis
Treatment with dose-adjusted EPOCH with rituximab has shown an eight-year survival rate of 91% for low-risk, 90% for low-intermediate-risk, 67% for high-intermediate-risk, and 31% for high-risk cases with few of the side effects associated with Burkitt lymphoma chemotherapy.
Epidemiology
Of all cancers involving the same class of blood cell, 2.3% of cases are Burkitt lymphoma. Epstein-Barr virus infection is strongly correlated with this cancer.
Gene targets
Unique genetic alterations promote cell survival in Burkitt lymphoma, distinct from other types of lymphoma. These TCF3 and ID3 gene mutations in Burkitt correspond to a cell survival pathway that may be found to be amenable to targeted therapy.